
There are irregular medium-sized nests of uniform round cells dissecting into the muscular wall of the appendix.
.', 'micro', '')){kind=link}
A different case shows a nested proliferation of bland cells with pale cytoplasm immediately under the acute inflammation of appendicitis.
){kind=link}
The cells resemble histiocytes almost, as they are degenerating amongst the inflammation and hemorrhage of an acute appendicitis.
){kind=link}
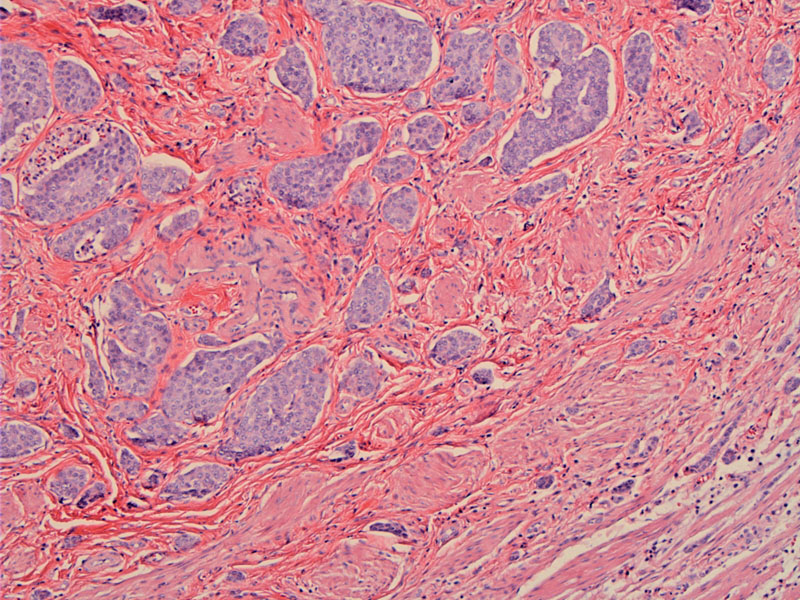
Another area shows that this is clearly a neoplastic process. The round to slightly jagged nests contain cohesive cells with a moderate amount of light pink to pale cytoplasm. The neuroendocrine nature of the lesion is more apparent here.
){kind=link}
Deeper within the wall one finds many lymphovascular channels with carcinoid within them.
){kind=link}
Carcinoid tumors (a.k.a. well-differentiated neuroendocrine tumor) are derived from resident endocrine cells in tissues. They can be found in virtually all organs, but the most common sites are the lungs and GI tract. In the GI tract, the appendix is the most common site, followed by the ileum, rectum, stomach and colon. Of note, the terminology these neoplasms is moving away from the usage of "carcinoid/atypical carcinoid/small cell carcinoma", and instead, "well-differentiated, moderately-differentiated and poorly-differentiated neuroendocrine carcinoma".
These tumors are often located at the tip of the appendix, sometimes obliterating the lumen. After fixation, they have a yellow color and are quite firm due to desmoplasia. Histologically, neoplastic cells with round nuclei and "salt and pepper" chromatin are arranged in islands, cords and sheets (Fletcher). Invasion of the muscle wall, lymph vessels and extension to the peritoneal surface are not uncommon (Rosai).
They can occur at any age with a peak incidence in the 3rd and 4th decade. Mostly, appendiceal carcinoids are incidental findings and the large majority are less than 1 cm in size (Rosai). The tumors are found in 0.3–0.9% of patients undergoing appendectomy (In't). Rarely, they may be associated with acute appendicitis due to obstruction of the lumen.
The behavior of the carcinoid depends on the anatomic site, depth of invasion, size and histologic features of necrosis and mitotic activity (Kumar). For example, appendiceal and rectal carcinoids rarely metastasize despite extensive local spread, whereas the majority (90%) of ileal, gastric and colonic carcinoids that have penetrated halfway through the muscularis will have metastasized.
Metastasis is rare, and if seen, are usually due to tumors exceeding 2 cm in diameter. Carcinoid syndrome secondary to appendiceal carcinoids is also exceptionally rare and usually secondary to liver metastasis (Rosai).
Tumors greater than 2 cm are also more likely to behave aggressively.
Benedix F, et al. Primary appendiceal carcinoma--epidemiology, surgery and survival: results of a German multi-center study. Eur J Surg Oncol. 2010 Aug;36(8):763-71.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 391.
In't Hof KH, et al. Carcinoid tumour of the appendix: an analysis of 1,485 consecutive emergency appendectomies. J Gastrointest Surg. 2008 Aug;12(8):1436-8.
Kumar V, Abbas AK, Fausto N. Robbins and Cotran Pathologic Basis of Disease. 7th Ed. Philadelphia, PA: Elsevier; 2005: 866-7.
McGory ML, et al. Malignancies of the appendix: beyond case series reports. Dis Colon Rectum. 2005 Dec;48(12):2264-71.