
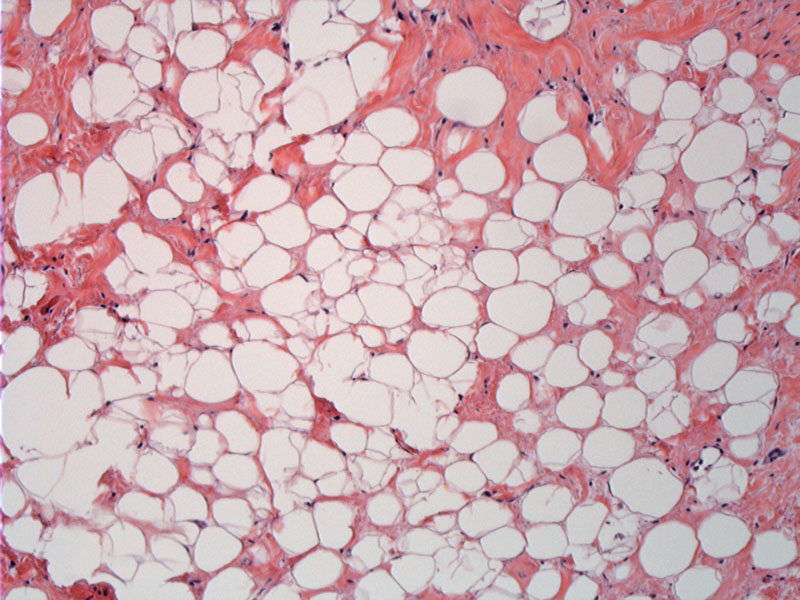
Admixture of mature fat is seen along with some fibrotic areas. This area is typical of the adipocytic (lipoma-like) subtype.
){kind=link}
Hyperchromatic stromal cells are scattered in the more fibrotic areas.
){kind=link}
Occasional slightly atypical nuclei are seen.
){kind=link}
Liposarcoma is the most common soft tissue sarcoma and is divided into three broad categories: (1) well-differentiated (2) myxoid (3) pleomorphic. The well-differentiated group is further divided into four subtypes: adipocytic (lipoma-like), sclerosing, inflammatory, and spindle cell. Dedifferentiated liposarcoma is considered by some to be a variant of well-differentiated liposarcoma, as it demonstrates well-differentiated areas transitioning to a high grade sarcoma (Fletcher).
Grossly, they resemble lipomas and are well circumscribed. The cut surface is yellow in the predominantly lipoma-like variant and white-grey in the more fibrous areas. The presence of multivacuolated lipoblasts have historically been considered the key feature of liposarcomas, but they are not the sole criteria because lipoblasts can be seen other benign lipomatous tumors such as lipoblastoma and pleomorphic lipoam (Folpe).
In well-differentiated liposarcoma, the adipocytes show some variation in size (versus similar size in benign lipomas) and some will have hyperchromatic atypica nuclei. Scattered bizarre multinucleated stromal cells may be seen in the fibrous septae separating the fat lobules.
Karyotypes of liposarcomas have shown that they typically have ring or giant marker chromosomes on the long arm of chromosome 12. These rings contain copies (amplification) of several proto-oncogenes such as MDM2, CDK2, HMGA2, SAS, GLI, DDT13, OS1 and OS9 (Folpe).
Staining for MDM2 and CDK4 may be helpful in identifying well-differentiated liposarcomas and is in fact, more consistently positive in dedifferentiated liposarcoma (Fletcher).
Liposarcomas typically occur in adulthood, with a peak incidence in the 5th through 7th decades. Liposarcomas are very rare in childhood and if present, occur between the ages of 10-15 and are of the myxoid subtype.
Usually, the history of a long-standing mass is present. But rapid growth can indicate dedifferentiation or the evolution of a myxoid liposarcoma to its high-grade form (round cell type).
Surgery is the mainstay of therapy and the only approach offering the potential of cure.
Survival at 5 years for well-differentiated liposarcoma is 90%. At 10 years, it drops to 60%, most likely due to retroperitoneal tumors that are difficult to resect and thus, recur. For dedifferentiated liposarcomas, a similar pattern exists, where the 5 year survival is 60-70% and dropping to 40-50% in 10 years due to recurrence of retroperitoneal tumors (Fletcher).
→Well-differentiated liposarcomas come in four major subtypes: lipoma-like, sclerosing, inflammatory and spindle-cell.
→They arise mainly in the limbs and retroperitoneum. The sclerosing variant is predominantly centered in the retroperitoneum.
→Liposarcomas characteristically exhibit ring chromosomes on the long arm of chromosome 12, which contain MDM2 and CDK2 proto-oncogenes, among others.
→Prognosis depends on the site. Retroperitoneal locations are difficult to resect and thus may recur.
• Lipomatous : Liposarcoma, Pleomorphic Type
• Lipomatous : Liposarcoma, Dedifferentiated Type
• Lipomatous : Well-differentiated liposarcoma, Sclerosing Fibroinflammatory Variant
• Lipomatous : Liposarcoma, Pleomorphic Type
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 1534-1539..
Folpe AL, Inwards CY. Bone and Soft Tissue Pathology: Foundations in Diagnostic Pathology Philadelphia, PA: Elsevier; 2010: 108-112.