
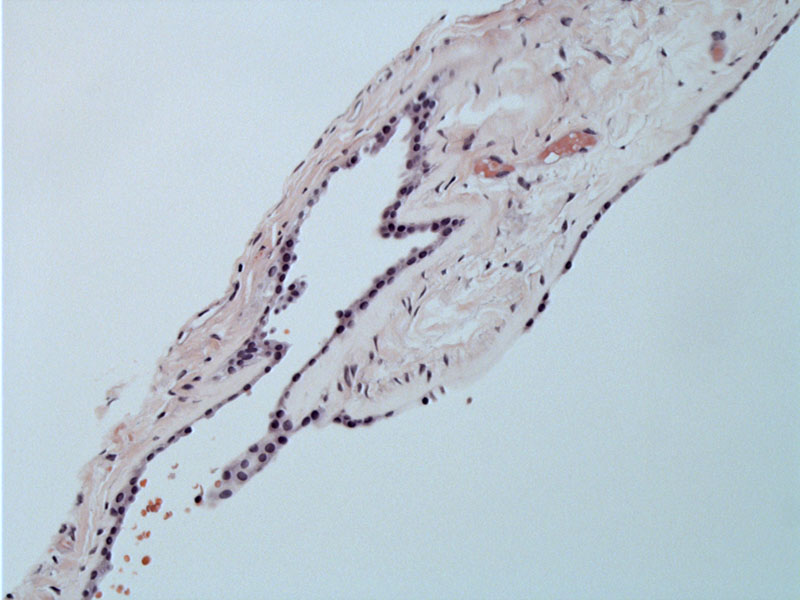
The cyst has a thin fibrous capsule lined with a single layer of epithelium and contains gelatinous material. The epithelium can range from cuboidal to ciliated columnar to goblet cells.
Here the eosinophilic colloid material filling the cyst can be appreciated.
Colloid cysts of the third ventricle are non-neoplastic lesions, however, they arise in the roof of the third ventricle and can obstruct the foramina of Monro. This can lead to noncommunicating hydrocephalus, a potentially fatal condition (Kumar).
Grossly, these cysts contain thick gelatinous material derived from breakdown of epithelium and secretions. Cysts range from 3 to 40 mm, and size does not predict clinical behavior since a small cyst can lead to sudden death (Amy).
Colloid cysts account for approximately 1% of intracranial tumors and may be of neuroectodermal origin, although this is disputed (Amy).
They can arise at any age. Due to impaired CSF flow and hydrocephalus, positional headaches are common symptoms. Other manifestations include sudden paralysis of lower extremities, incontinence, personality changes, gait disturbance, and rarely, sudden death (Prayson, Amy).
Depending on size, location and clinical symptoms, treatment includes observation with serial imaging, shunting (to divert CSF flow), stereotactic aspiration and resection of cyst. Removal of the cyst via microsurgical techniques is the gold standard (Amy).
Amy C, Walker E. Not just Another Headache: Colloid Cyst of the Third Ventricle. The Nurse Practitioner (2003), Vol 28 (9); 8-12.
Kumar V, Abbas AK, Fausto N. Robbins and Cotran Pathologic Basis of Disease. 7th Ed. Philadelphia, PA: Elsevier; 2005: 1406.
Prayson, RA. Neuropathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elvesier; 2005: 519-20.

){kind=link}
){kind=link}