
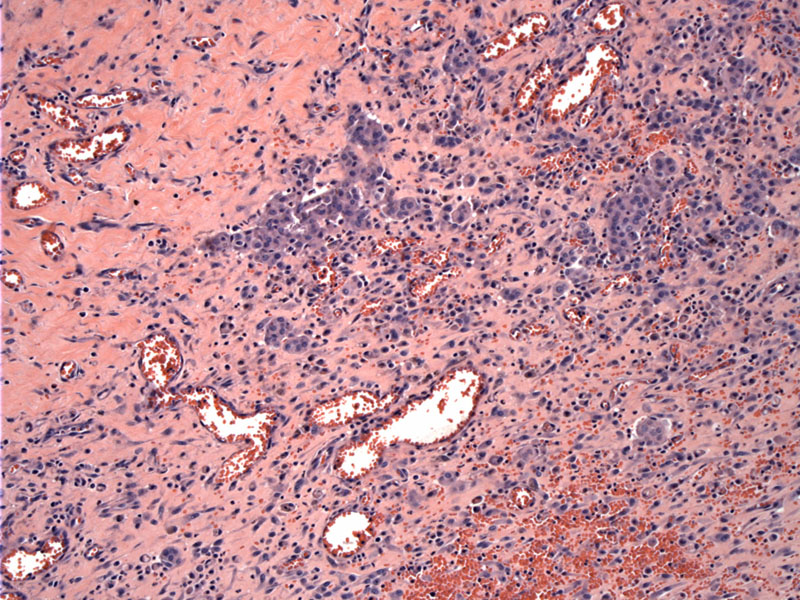
Organizing pleuritis is seen here with entrapped mesothelial cells. Zonation is a feature of a benign reactive process.
Vascular proliferation, chronic inflammation and fibrosis form an clearly reactive picture.
There an admixture of chronic inflammation, vascular spaces and fibrin deposition. Small nests of mesothelial cells are entrapped within this proliferation.
Bland small aggregates of mesothelial cells form cleft like spaces, embedded in a fibroinflammatory background. More cellular lesions are actually a feature which favors a benign process.
At higher power, the mildly atypical mesothelial cells have prominent nucleoli.
This is a peel (or rind) from the pleura, consisting of fibrosis and a coating of reactive mesothelial cells. Tangential sectioning may give false impression of invasion.
A higher power of this area reveals only mildly atypical mesothelial cells in a multilayered arrangement. Invasion is lacking.
A corresponding area is strongly positive for keratin 5/6 within the sequestered mesothelial cells. Keratin staining can be helpful in highlighting the distribution of mesothelial cells, but cannot distinguish between hyperplasia and malignancy.
Mesothelial hyperplasia and organizing pleuritis are common reactions to inflammation and chronic effusions. These entities must be distinguished from malignant mesothelioma, however, this may be difficult since biopsies often provide scant material and there is no specific IHC marker that separates benign mesothelial reactions from malignant mesothelioma (Henderson).
Mesothelial hyperplasia can assume a variety architectural patterns including tubular, papillary, tubulopapillary, solid and trabecular. In mesothelial hyperplasia, the papillae and tubular structures are simple, whereas in malignant mesothelioma or atypical mesothelial hyperplasia, the tubules and papillae tend to be branching and more complex (Cagle).
Reactive mesothelial proliferations, especially when mesothelial cells are entrapped within stroma, can mimic invasive or metastatic epithelial tumors. For example, mesothelial hyperplasia, often seen in the mesothelium covering the adnexa and ovary of women with salpinigits, endometriosis or ovarian tumors, can mimic invasive tumor (Fletcher).
Mesothelial cells may be polygonal and their appearance may be bland or atypical. Multinucleated giant cells and mitotic figures can also be seen. Histiocytes may be prominent component and distinguishing between the two types of cells (histiocytes vs mesothelial cells) may require IHC (Fletcher).
To summarize, features seen in mesothelial hyperplasia as well as malignant mesothelioma include cytologic atypia, mitotic figures, necrosis, papillary tufts, simple tubular formations and entrapment of mesothelial cells. Features that favor a diagnosis of malignant mesothelioma include unequivocal invasion of underlying tissues, full thickness cellularity of the pleura (without zonation), bland necrosis without accompanying inflammation, complex branching papillae and tubules, atypical mitoses and significant pleomorphism (Cagle).
Unless obvious invasion is seen on a biopsy, it may be prudent to employ the term "atypical mesothelial hyperplasia" when obvious invasion is not present -- and wait for more tissue!
Common areas affected by mesothelial hyperplasia aside from the pleura and peritoneum include the mesothelial-lined adnexa and ovary as well as hernia sac.
A biopsy of atypical mesothelial cells along with a history of asbestos exposure should not automatically trigger a diagnosis of malignant mesothelioma. Absbestos exposure is far more likely to cause absestosis, pleural effusions, benign pleural plaques and mesothelial hyperplasia(Cagle).
→Benign reactive lesions of the mesothelium, namely mesothelial hyperplasia and fibrinous pleuritis, must be distinguished from malignant mesothelioma.
• Pleura : Mesothelioma, Epithelioid Type
• Pleura : Mesothelioma, Desmoplastic Type
Cagle PT, Churg A. Differential diagnosis of benign and malignant mesothelial proliferations on pleural biopsies. Arch Pathol Lab Med. 2005 Nov;129(11):1421-7.
Churg A, Cagle P, Colby TV, Corson JM, Gibbs AR, Hammar S, Ordonez N, Roggli VL, Tazelaar HD, Travis WD, Wick M. The fake fat phenomenon in organizing pleuritis: a source of confusion with desmoplastic malignant mesotheliomas. Am J Surg Pathol. 2011 Dec;35(12):1823-9.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 881-2.
Henderson DW, Shilkin KB, Whitaker D. Reactive mesothelial hyperplasia vs mesothelioma, including mesothelioma in situ: a brief review. Am J Clin Pathol. 1998 Sep;110(3):397-404.

){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}