
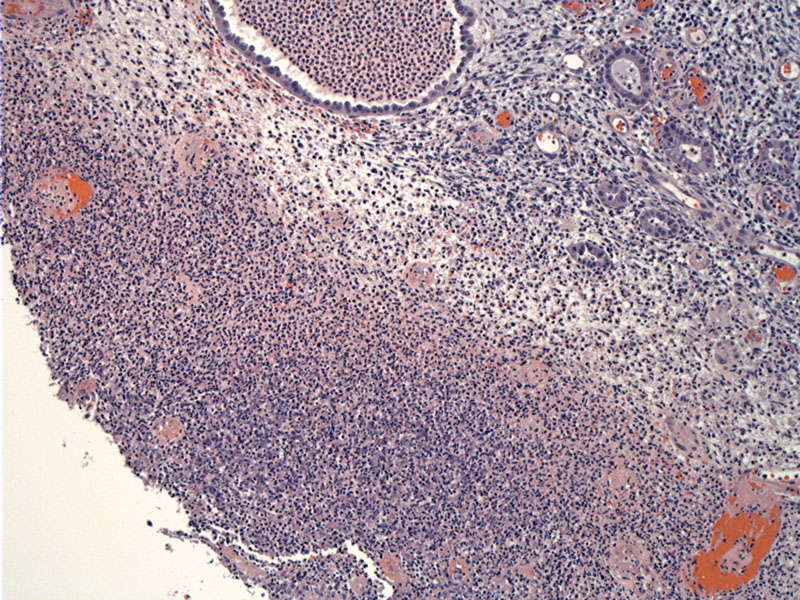
This is a polypoid lesion arising within the endometrium, thus the endometrium undergoes surface mechanical trauma. Exudative debris lines the surface.
){kind=link}
There is an irregular interface with the underlying myometrium due to invasion. Only about 15% of all adenosarcomas invade into myometrium, which is usually limited to the inner half. However, adenosarcoma with sarcomatous overgrowth may be associated with deep myometrial and vascular invasion. The myoinvasive component usually contains both the epithelial and stromal elements.
){kind=link}
Bland irregular shaped glands are embedded within a highly cellular stroma. The stromal cells are markedly atypical and include a fair number of bizarre multinucleated ones.
){kind=link}
Numerous mitoses and atypical forms are found. The cells are slightly spindled but also may contain multiple nuclei.
){kind=link}
There is variable edema to the stroma imparting a loose appearance to the neoplasm. Mitotic figures easily stand out.
){kind=link}
The stroma is extensive and comprises the majority of the tumor mass in this type of adenosarcoma. Extremely bizarre nuclei scattered cells are found within it.
){kind=link}
Variation in stromal cellularity is a feature, with prominent periglandular cuffing of the stroma characterized by increased cellularity immediately beneath the epithelium.
){kind=link}
An essential feature is that the epithelial element is benign with a malignant mesenchymal component. The epithelium in most cases is endometrioid in type, although ciliated, mucinous, and occasionally squamous type may also be found. The epithelium is often active, with mitoses present.
){kind=link}
Adenosarcomas in which > 25% of the tumor consists of pure sarcoma are designated as “adenosarcoma with sarcomatous overgrowth”(Clement). The areas of sarcomatous overgrowth often comprise much more than 25% of the neoplasm and are usually composed of areas resembling undifferentiated sarcoma. Heterologous components may be found in the sarcomatous areas.
These may arise in all age groups, but are usually seen in post-menopausal women. The most common presenting symptom is abnormal vaginal bleeding. Pelvic pain, an abdominal mass, or vaginal discharge may also be found (MuCluggage).
Hysterectomy with bilateral salpingo-oophorectomy is the mainstay of therapy. Overall, as the disease is rare, adjuvant radiation therapy and/or chemotherapy has not been adequately evaluated, with some studies containing small numbers of patients showing benefit and some showing none.
Adenosarcomas with sarcomatous overgrowth harbors a poor prognosis and may be associated with deep myometrial invasion or distant metastasis. Studies show a propensity for uterine adenosarcomas with sarcomatous overgrowth to recur and metastasize even with early-stage disease in a manner similar to carcinosarcoma (Krivak).
In one study, survival was only 63–69% for women whose tumors invaded into the wall of the uterus and lower than 50% for disease beyond the uterus (Arend). Advanced age has been associated with a worse prognosis in one study (Arend).
Depth of invasion into the myometrial wall is an important prognostic indicator.
• Endometrium : Adenosarcoma, Low Grade
• Endometrium : Mixed Malignant Mullerian Tumor
• Endometrium : Atypical Polypoid Adenomyoma
Arend R,et al. Long-term outcome and natural history of uterine adenosarcomas. Gynecol Oncol. 2010 Aug 3.
Clement PB. Adenosarcomas of the uterus with sarcomatous overgrowth. A clinicopathologic analysis of 10 cases. Am J Surg Pathol. 1989;13:28–38.
Krivak TC, Seidman JD, McBroom JW, MacKoul PJ, Aye LM, Rose GS. Uterine adenosarcoma with sarcomatous overgrowth versus uterine carcinosarcoma: comparison of treatment and survival. Gynecol Oncol. 2001 Oct;83(1):89-94.
McCluggage. Mullerian adenosarcoma of the female genital tract. WG. Adv Anat Pathol. 2010 Mar;17(2):122-9.