System: Gastrointestinal: Small Intestines: Neoplastic: Ampullary Adenoma with Mucinous Adenocarcinoma

System: Gastrointestinal: Small Intestines: Neoplastic: Ampullary Adenoma with Mucinous Adenocarcinoma

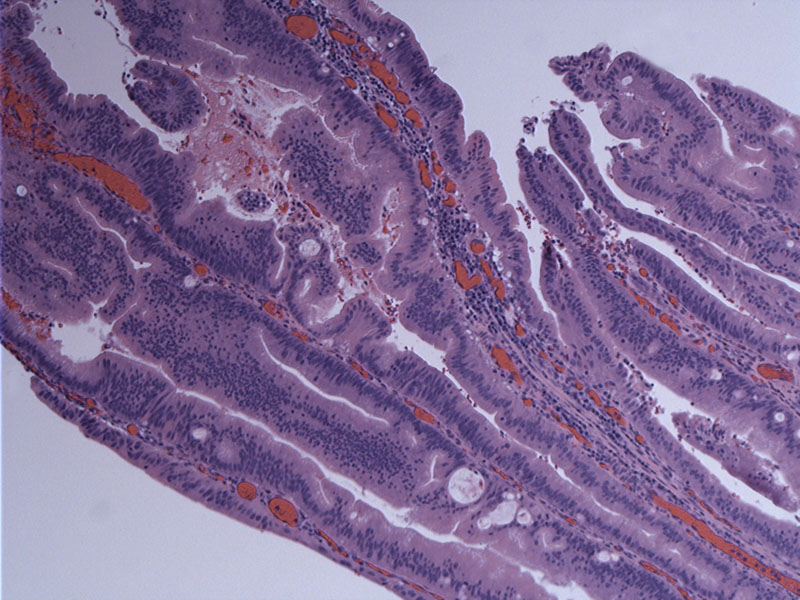
A portion of the mucosal surface shows the remainder of a villous adenoma. Long slender villous projections with pseudostratified nuclei are appreciated.
Directly underlying the adenomatous portion is the development of invasion. Morphologically, small intestinal tumors are identical to their colonic counterparts. However this particular example is of a mucinous adenocarcinoma.
This particular tumor shows abundant mucin production which is largely extracelluar. Most colloid carcinomas of the pancreas and periampullary region arise in association with a well-defined in situ papillary neoplasm. The finding of duodenal villous adenoma in this case favors a duodenal primary.
Copious extracellular mucin forms large pools, with malignant cells aggregates scattered within the pool.
This periampullary tumor involves the duct.
Small intestinal adenomas usually involve the duodenum and are solitary. Small intestinal adenocarcinomas are also most common in the duodenum, where about two-thirds involve the periampullary region. The exception to this distribution is Crohns disease, in which there is a preference for the ileum.
Periampullary adenocarcinomas generally arise from pre-existing villous adenomas. Grossly, they are exophytic and bulge into the lumen of the duodenum. It is important to differentiate between ampullary or periampullary adenocarcinoma, which arise from intestinal mucosa covering the ampulla, from carcinoma of the pancreas or distal third of the common bile duct. In cases of advanced disease, it may not be possible to make this distinction and thus, one can employ the all-encompassing term "carcinoma of the pancreato-biliary-ampullary region" (Rosai).
Histologically, there may be a superficial papillary component with an appearance similar to a villous adenoma with an underlying invasive component.
Most patients are over the age of 60 with a slight male predominance (Rosai). Some cases may be associated with FAP and neurofibromatosis type I (Rosai, Fletcher).
Commonly presents with abdominal pain, obstruction and GI bleeding. Obstructive jaundice may be evident in those with ampullary involvement. Presentation at an advanced stage is not uncommon. Early carcinomas may not be detectable endoscopically, but ultrasound and CT may show dilatation of the pancreatic duct or the common bile duct (Rosai).
Surgery is the mainstay of therapy. Chemoradiation plays little role.
Colloid carcinomas of the periampullary region do not necessarily have a better prognosis than conventional carcinomas. Factors such as tumor location, perineural invasion, vascular invasion, and margin status after resection are of primary importance (Seidel).
• Small Intestines : Adenocarcinoma (Jejunum)
• Pancreas : Intraductal Papillary Mucinous Neoplasm
Seidel G,et al Almost all infiltrating colloid carcinomas of the pancreas and periampullary region arise from in situ papillary neoplasms: a study of 39 cases. Am J Surg Pathol. 2002 Jan;26(1):56-63.
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}