System: Serosal Membranes: Pleura: Neoplastic: Mesothelioma, Desmoplastic Type

System: Serosal Membranes: Pleura: Neoplastic: Mesothelioma, Desmoplastic Type

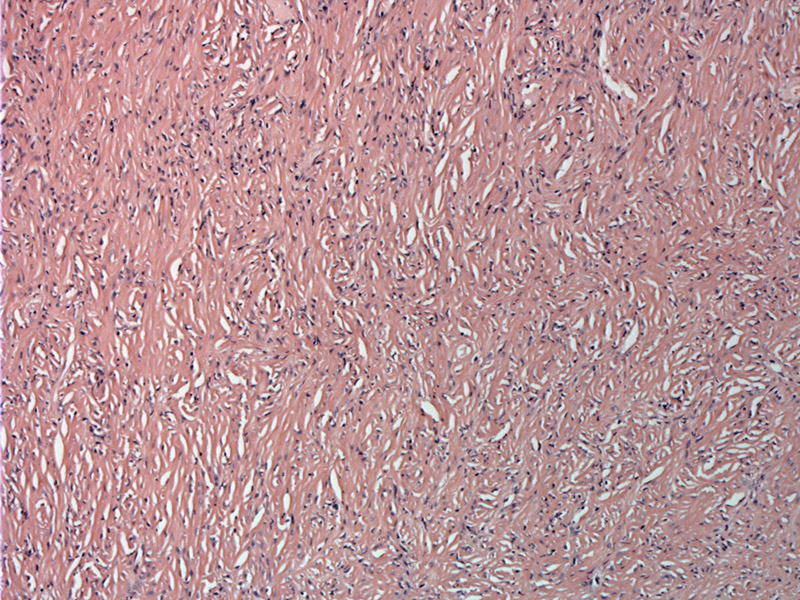
This desmoplastic mesothelioma is paucicellular with prominent collagenization. There is a vaguely fasicular pattern of growth.
Here is a more cellular area with a modest lymphocytic infiltrate.
Here is a more collagenized area; one can see how this variant may be mistaken for fibrous pleuritis.
Elongated moderately pleomorphic tumor cells are present in the interstices between collagen bundles - a patternless pattern.
The area of tumor on the left transitions to bland necrosis in the middle and right field. Bland necrosis is a fairly well demarcarted area that appears more pink, less cellular and has little to no karrhyorhexis. Note that the underlying tissue pattern remains intact and there is no inflammatory response. Bland necrosis is a fairly reliable feature of malignancy.
Capillaries in desmoplastic mesotheliomas tend to be inconspicuous and arranged in a haphazard fashion (Cagle).
The more cellular areas tend to exhibit pleomorphism with prominent nucleoli -- the cells are overtly sarcomatous.
A storiform pattern is seen in this more cellular area.
Invasion into fat is an unequivocal sign of malignancy.
The sarcomatoid variant of mesothelioma consists of storiform or fascicular proliferations of spindle cells, thus mimicking fibrosarcomas or so-called malignant fibrous histiocytomas (Fletcher). The malignant cells have scant cytoplasm and occasionally prominent nucleoli. When stromal collagen deposition is prominent, the tumor is called the desmoplastic variant of sarcomatoid mesothelioma, which can have a deceptively bland, fibrous appearance strikingly similar to fibrous pleuritis (pleurisy).
While it is true that there is a strong association between exposure to some types of asbestos and mesothelioma, cohorts of workers with heavy asbestos exposure also have an increased incidence of lung carcinoma, a tumor that frequently spreads to the pleura, and an increased incidence of a variety of benign pleural processes, such as plaques, diffuse fibrosis, effusion, and rounded atelectasis (Churg). Overall, benign pleural diseases are actually more common than malignant ones in asbestos workers. Identification of stromal invasion is the most reliable criterion of mesothelial malignancy. Thus, the pathologist must insist on adequate sampling by the surgeon.
• Pleura : Mesothelioma, Biphasic Type
• Pleura : Mesothelioma, Epithelioid Type
• Pleura : Solitary Fibrous Tumor
• Pleura : Fibrinous Pleuritis
Cagle PT, Churg A. Differential diagnosis of benign and malignant mesothelial proliferations on pleural biopsies. Arch Pathol Lab Med. 2005 Nov;129(11):1421-7.
Churg A, Colby TV, Cagle P, Corson J, Gibbs AR, Gilks B, Grimes M, Hammar S, Roggli V, Travis WD. The separation of benign and malignant mesothelial proliferations. Am J Surg Pathol. 2000 Sep;24(9):1183-200.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 206-7.
Mangano WE, Cagle PT, Churg A, Vollmer RT, Roggli VL. The diagnosis of desmoplastic malignant mesothelioma and its distinction from fibrous pleurisy: a histologic and immunohistochemical analysis of 31 cases including p53 immunostaining. Am J Clin Pathol. 1998 Aug;110(2):191-9.
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}