
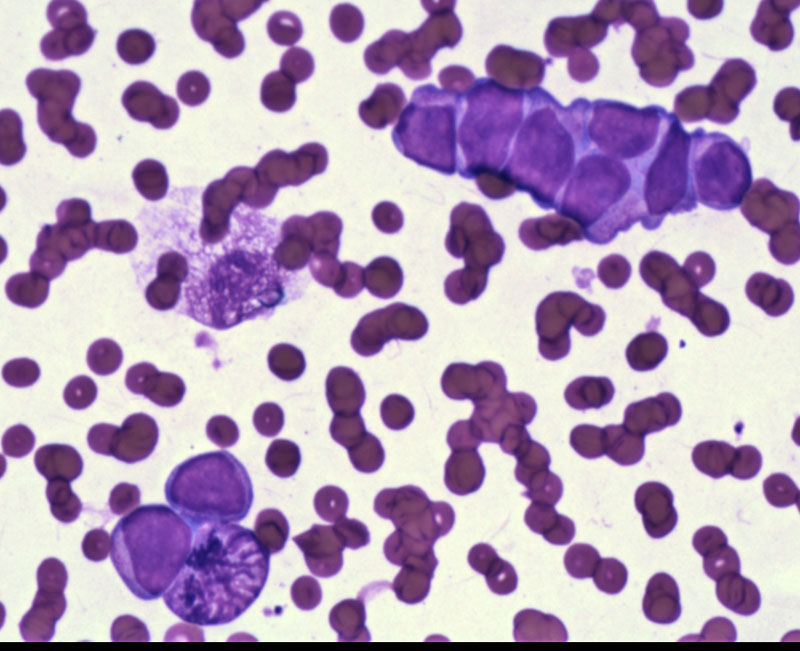
Case 1 - This Diff-Quik image demonstrates a linear groups of cells with nuclear molding. There is only a thin rim of cytoplasm while enlarged nuclei occupies most of the cells. The chromatin is relatively uniform and nucleoli are not prominent.
){kind=link}
FNA shows dispersed single uniform cells within a background of many apoptotic cells. The features are similar to that of pulmonary small cell carcinoma.
){kind=link}
Round cells with uniform speckled chromatin without distinct nucleoli suggest a neuroendocrine phenotype.
){kind=link}
Cytokeratin 20 shows perinuclear dot-like positivity. Merkel cells have intermediate filaments arranged in whorled bundles around the nucleus, leading to the perinuclear dot-like staining when using LMWKs such as 8, 18, 19, 20. CK 20 is the most sensitive and specific for Merkel cells. Unlike Merkel cell carcinoma, cytokeratin 20 with dot-like positivity is not seen in small cell carcinoma of the lung.
){kind=link}
Merkel cell carcinomas consist of a monotonous proliferation of small round cells. These cells can occasionally infiltrate into subcutaneous fat or involvement of the epidermis, which can bring up the differential diagnosis of small cell carcinoma of the lung or malignant lymphomas.
){kind=link}
A common pattern of growth is the trabecular pattern. Merkel cell carcinomas can even form pseudorosettes at times, but this is not evident here.
){kind=link}
The nuclei are round and vesicular. Note that what you might initially mistaken for neutrophils are actually numerous mitotic figures and apoptotic bodies.
){kind=link}
Case 2 - Another (rather fuzzy) image demonstrating involving of the dermis by a dark blue infiltrate.
){kind=link}
At higher power, you can see that the epidermis is spared i.e. forming a Grenz zone.
){kind=link}
Dark uniform cells infiltrate the dermis in cords and nests.
){kind=link}
The tumor cells are darkly stained, but you can still make out the speckled chromatin pattern. The insular growth pattern is also typical of neuroendocrine tumors.
){kind=link}
Here is a beautiful IHC panel. Note that MAK6 is an anti-cytokeratin antibody.
){kind=link}
Staging system for Merkel Cell Carcinoma.
){kind=link}
Merkel cell carcinoma (MCC) is a rare aggressive neuroendocrine neoplasm of the skin. 400 cases diagnosed in the US each year, and it has a higher mortality rate compared to melanoma (Bickle).
MCC demonstrate both epithelial and neuroendocrine differentiation. It is currently thought that MCC make not arise from Merkel (neuroendocrine) cells after all, but rather a primitive stem cell capable of differentiating toward various cell lines (Calder).
Interestingly, a new polyomavirus (Merkel cell polyomavirus, MCV) has been isolated in 80% of Merkel cell carcinomas (versus 16% in normal skin), thus, the possibility that viral infection is involved in the pathogenesis is being considered (Feng).
The lesion is usually located within the dermis, with the overlying epidermis uninvolved. However, Merkel cells can involve the epidermis. Rarely, the lesion can be confined to the epidermis (MCC in situ). Merkel cell carcinomas can be seen in conjunction with squamous cell carcinoma.
IHC reveal that MCC demonstrate both epithelial and neuroendocrine differenitation. There is characteristic perinuclear "dot-like" reactivity for low molecular weight keratins such as CK20, AE1/AE3 or CAM5.2. This dot-like pattern can also be seen in neurofilament stains. Other positive markers include EMA, NSE, chromogranin and BER-EP4 (Fletcher).
MCC should be differentiated from small cell carcinoma from lung, or malignant lymphomas that involve the skin. IHC panels will be helpful as MCC is negative for CK7 and TTF-1, whereas SCC of the lung is positive for these markers as well as being negative for CK20 (Calder).
These rare aggressive neuroendocrine tumors generally occur in the elderly (mean age at diagnosis is 75). Immunosuppression (e.g. HIV infection, CLL, post-organ transplant) is also a risk factor.
There is no sex predilection. Whites are 20x more likely than blacks to be affected. Fair skin, sun exposure, and decreased immunity appear to be risk factors. Clinically seen
as a red dome-shaped nodule which can be ulcerated, mimicking a basal cell carcinoma. The face, neck and extremities (sun-exposed regions) are the most common locations.
Surgery with clear margins is recommended. However, at the time of presentation, many cases have regional nodal metastases and lymphovascular invasion. Chemotherapy or radiation has not proven to improve survival.
Clinical stage is the most important prognostic factor. Patients with localized disease often have an indolent course with local excision alone. On the other hand, many tumors are aggressive and have a tendency for regional recurrence and distant metastases.
Overall, this is an aggressive tumor with poor prognosis. For example, in a study of 185 patients with MCC, 22% with localized disease died and 54% with nonlocalized diseased died. After 5 years, the mortality rate increased to 55% and 84% respectively (Kaae).
Merkel cell carcinoma is a tumor of older individuals and has a predilection for the immunosuppressed
• Spleen : Diffuse Large B Cell Lymphoma
• Melanocytic : Melanoma, Nodular Type
Bickle K, Glass LF, Messina JL et al. Merkel cell carcinoma: a clinical, histopathologic, and immunohistochemical review. Semin Cutan Med Surg. 2004 Mar;23(1):46-53.
Calder KB, Smoller BR. New insights into merkel cell carcinoma. Adv Anat Pathol. 2010 May;17(3):155-61.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 1466.
Kaae J, Hansen AV, Biggar RJ et al. Merkel cell carcinoma: incidence, mortality, and risk of other cancers. J Natl Cancer Inst. 2010 Jun 2;102(11):793-801. Epub 2010 Apr 27.
Rosai, J. Rosai and Ackerman's Surgical Pathology. 9th Ed. Philadelphia, PA: Elsevier; 2004: 177-9.