
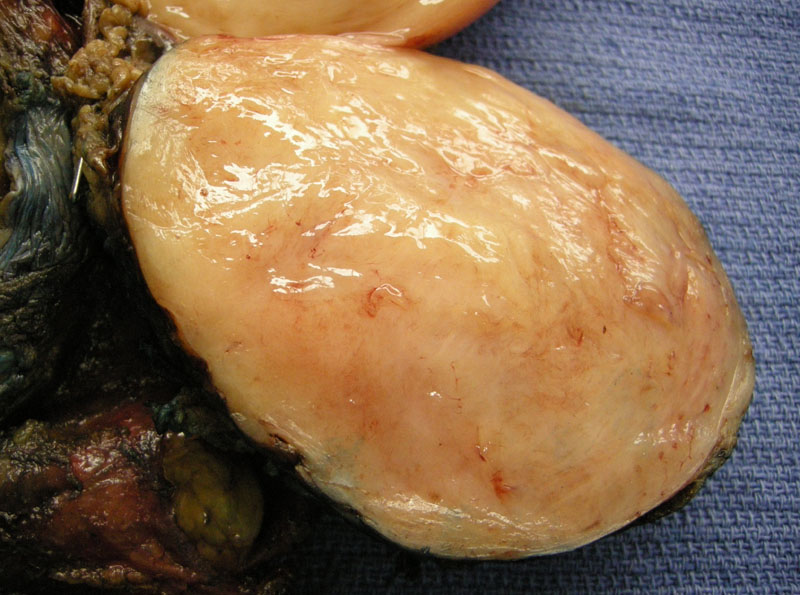
The cut surface has a tan cut trabeculated surface, resembling a fibroid.
){kind=link}
Ganglioneuroma shows a spindle cell background with scattered mature ganglion cells.
){kind=link}
Neuroblastoma, ganglioneuroblastoma, and ganglioneuroma are related tumors arising from neural crest cells and can be seen in sites where sympathetic tissue exist e.g. mediastinum, retroperitoneum, pelvis, head and neck and adrenal gland. These three tumors differ in their maturation (Allende, Longergan). The most mature tumor is ganglioneuroma, consisting of mature ganglion cells and mature stroma -- these tumors behave in a benign fashion. Ganglioneuroblastoma takes an intermediate position and is composed of mature ganglion cells as well as immature neuroblasts. Neuroblastoma is the most immature and undifferentiated of the group. Note that the behavior of neuroblastomas can vary widely. Neuroblastomas with certain clinicopathologic features (e.g. favorable histology, age of patient, DNA content) may pursue a benign course (Longergan).
Most cases of ganglioneuromas arise in the posterior mediastinum and retroperitoneum. ~ 30% of these tumors occur in the adrenal gland (Allende). Grossly, the tumor is well-circumscribed and firm with a smooth glistening surface or sometimes a whorled trabeculated surface reminiscent of a fibroid leiomyoma (Fletcher).
Histologically, variable numbers of mature gangliocytes (ganglion cells) are seen in a background of spindle cells resembling a Schwannian matrix. The ganglion cells may occasionally contain a granular pigment, likely lipofuscin or neuromelanin (Fletcher).
Ganglioneuromas of the posterior mediastinum and retroperitoneum tend to occur in younger patients whereas ganglioneuromas of the adrenal gland arise in the 4th and 5th decades of life (Allende, Chen). These tumors are usually asymptomatic and found incidentally on imaging. If they release catecholamines, labile hypertension and flushing may be seen.
For tumors of the posterior mediastinum, surgery is advocated because although these tumors are benign, they may compress or invade local nerves and mediastinal structures. Given this potential, these tumors are resected.
Ganglioneuromas do not recur following resection and are not metastatic.
• Adrenal : Neuroblastoma (Case 2)
Allende DS, Hansel DE, MacLennan GT. Ganglioneuroma of the adrenal gland. J Urol. 2009 Aug;182(2):714-5. Epub 2009 Jun 18.
Chen CL, Huang ST, Chang PL, Ng KF. Adrenal ganglioneuroma: report of five cases. Chang Gung Med J. 2000 Sep;23(9):550-4.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 1777-8.
Lonergan GJ, Schwab CM, Suarez ES, Carlson CL. Neuroblastoma, ganglioneuroblastoma, and ganglioneuroma: radiologic-pathologic correlation. Radiographics. 2002 Jul-Aug;22(4):911-34.
***Gross image courtesy of Myra Zucker, Dept of Pathology at University of New Mexico, Albuquerque NM.