System: Hematopathology: Bone Marrow: Reactive: Zinc-induced Copper Deficiency

System: Hematopathology: Bone Marrow: Reactive: Zinc-induced Copper Deficiency

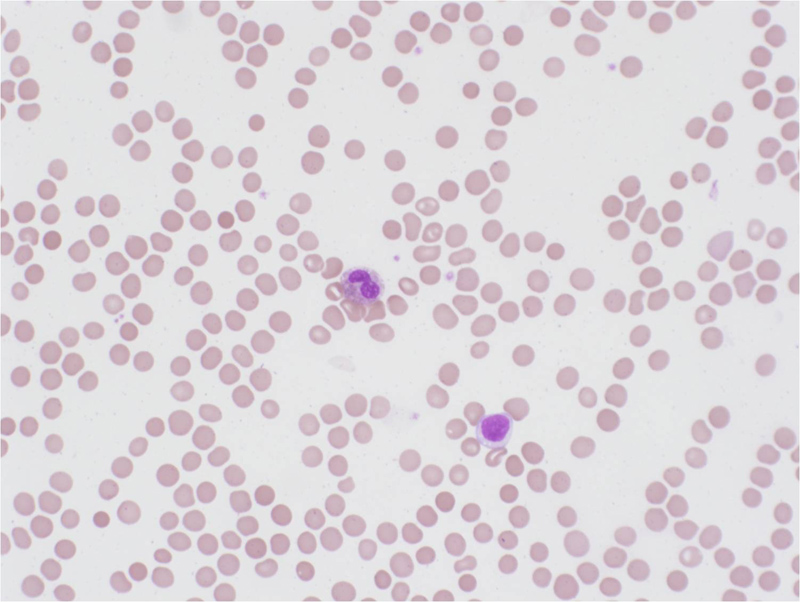
The peripheral smear usually shows evidence of anemia, neutropenia, and a normal platelet count. Often there is hypogranularity and hypolobation of the myeloid lineage.
The bone marrow aspirate commonly shows a left shift in the myeloid lineage and vacuolization of the myeloid and erythroid precursors.
High power view of the bone marrow aspirate shows vacuolization of myeloid and erythroid precursors next to each other.
Trephine core biopsy is morphologically unremarkable and does not show features commonly seen in MDS such as dysmegakaryopoiesis.
Copper deficiency is a rare and under-recognized cause of sideroblastic anemia and neutropenia. It has a distinctive morphologic presentation characterized by cytoplasmic vacuolization in erythroid and myeloid precursors as well as ringed sideroblasts on bone marrow examination. These findings may be concerning for an underlying myelodysplastic process at initial evaluation by the pathologist. According to the “Hemepath Bible” (WHO Classification) it is imperative that one excludes all non-clonal causes, such as in this case of zinc-induced copper deficience, before making the diagnosis of MDS.
The mechanism by which a zinc excess is thought to result in copper deficiency is by the indirect interaction between the two metals in the intestine (Cousins). Zinc excess may be the result from treating conditions like diarrhea, the common cold, and acne with zinc supplementation. Interestingly, there have been reports of zinc-induced copper deficiency secondary to denture adhesives (Nations et al). Other causes of copper deficiency include dietary deficiency, malabsorption, excess excretion, and Menkes syndrome (X-linked recessive mutation in ATP7A gene responsible for a protein involved in copper regulation).
Patients may present clinically with signs and symptoms of anemia (fatigue, elevated heart rate, shortness of breath, dizziness, pale skin) and/or neurologic dysfunction as a result from a neuropathy or myelopathy (paresthesia, ataxia, spasticity) (Kumar). Their laboratory findings typically show a normocytic or macrocytic anemia, neutropenia, and normal platelet count.
It is imperative to obtain a through history to identify possible causes of zinc excess.
Treatment involves removal of the source of excessive zinc and copper supplementation.
Typically there is resolution of symptoms after initiation of therapy.
Cousins RJ. Metallothionein — aspects related to copper and zinc metabolism. J Inherit Metab Dis. 1983;6:S15-21.
Kumar N, Gross J, Ahlskog J. Myelopathy due to copper deficiency. Neurology. 2003;61:273-4.
Nations SP, Boyer PJ, Love LA, et al. Denture cream: an unusual source of excess zinc, leading to hypocupremia and neurologic disease. Neurology. 2008;71:639-43.
Swerdlow SH, Campo E, Harris NL, et al., Eds. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, 4th Ed. Lyon: IARC Press; 2008:88-94.
Willis MS, Monaghan SA, Miller ML, et al. Zinc-Induced Copper Deficiency: A report of three cases initially recognized on bone marrow examination. Am J Clin Pathol. 2005;123:125-31.
){kind=link}
){kind=link}
){kind=link}
){kind=link}