
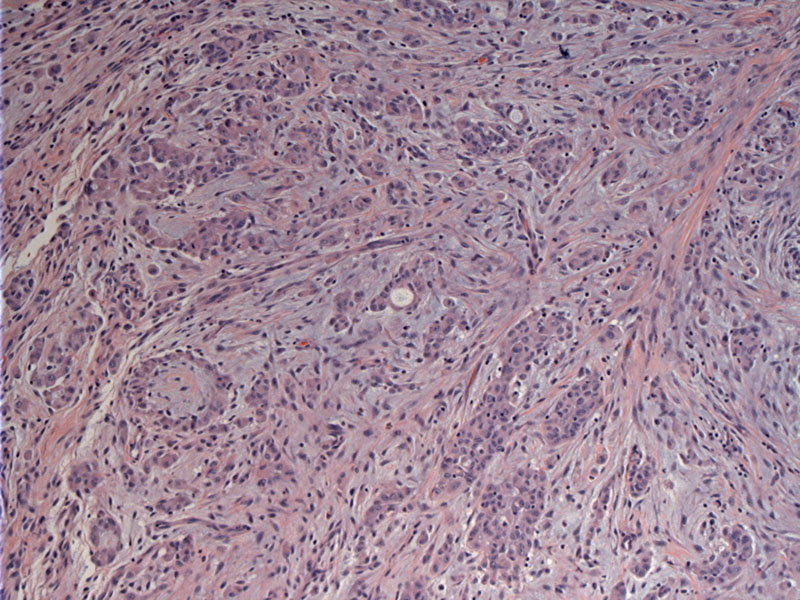
Nests of malignant cells invade through the peritoneum. The neoplastic cells are epithelioid and somewhat bland appearing.
){kind=link}
Cleft-like spaces, also seen in the pleural counterpart, can be appreciated. The most common histologic variant of peritoneal mesothelioma is epithelioid.
){kind=link}
Cytokeratin 5/6 is usually positive in mesotheliomas. Other positive stains include calretinin and thromobomodulin.
){kind=link}
D2-40 positivity is helpful in excluding ovarian serous carcinomas in female patients.
){kind=link}
WT1 is positive, however, serous carcinoma of the ovary would also show WT1 positivity. Therefore, an ER stain would be more useful as it is negative in mesotheliomas.
){kind=link}
The majority of malignant mesotheliomas are pleural, but 10-20% can be peritoneal. Peritoneal mesothelioma, an aggressive neoplasm strongly associated with asbestos exposure, shows rapid spread within the abdominal cavity, involving most accessible peritoneal and omental surfaces.
Peritoneal mesothelioma is usually not seen in women; in women, when encountered with a peritoneal neoplasm with malignant and papillary features, one should think about primary peritoneal carcinoma, also known as extraovarian papillary serous carcinoma OR papillary serous carcinoma of the ovary that has spread to the peritoneum (Fletcher).
Cumin found that h-caldesmon, calretinin, ER, and Ber-EP4 are the most useful markers in distinguishing epithelioid peritoneal mesothelioma from serous papillary carcinoma of the ovary. Calretinin is a good "positive" marker for mesothelioma and the other three are good "positive" markers for ovarian papillary serous carcinoma (Cumin).
Occurs most commonly in older men with a strong association with high levels of asbestos exposure; 50% also have pulmonary abestosis/fibrosis (Kumar). Presenting symptoms include abdominal discomfort, weight loss, ascites and digestive complaints.
Grossly, diffuse sheetlike or nodular thickening of the peritoneal surfaces are seen, but may occasionally forms a localized mass. Classifying malignant mesotheliomas into diffuse and localized subtypes has prognostic importance -- the diffuse type is highly aggressive but localized ones usually have a good prognosis following complete surgical excision of the lesions (Churg).
Microscopically, peritoneal mesotheliomas exhibit the same histologic subtypes seen in pleural counterpart, however, sarcomatoid and biphasic tumors are less common.
Management has evolved similarly to ovarian cancer treatment and involves multiple modalities including cytoreductive surgery, heated intraoperative intraperitoneal chemotherapy with cisplatin and doxorubicin, and early postoperative intraperitoneal paclitaxel.
In most cases, survival is less than 2 years after diagnosis. However, new aggressive multimodal treatment (debulking, chemotherapy and radiation) may extend survival time to more than 70 months (Hesdorffer).
• Pleura : Mesothelioma, Epithelioid Type
• Pleura : Mesothelioma, Biphasic Type
Churg A, Cagle PT, Roggli VL. Tumors of the serosal membranes. Silver Spring, Md: ARP, 2006.
Comin CE, Saieva C, Messerini L. h-caldesmon, calretinin, estrogen receptor, and Ber-EP4: a useful combination of immunohistochemical markers for differentiating epithelioid peritoneal mesothelioma from serous papillary carcinoma of the ovary. Am J Surg Pathol. 2007 Aug;31(8):1139-48.
Hesdorffer ME et al. Combined resection, intraperitoneal chemotherapy, and whole abdominal radiation for the treatment of malignant peritoneal mesothelioma. Am J Clin Oncol. 2008 Feb;31(1):49-54.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 887-8.
Kumar V, Abbas AK, Fausto N. Robbins and Cotran Pathologic Basis of Disease. 7th Ed. Philadelphia, PA: Elsevier; 2005: 769.
Takeshima Y, Amatya VJ, Kushitani K, Inai K. A useful antibody panel for differential diagnosis between peritoneal mesothelioma and ovarian serous carcinoma in Japanese cases. Am J Clin Pathol. 2008 Nov;130(5):771-9.