
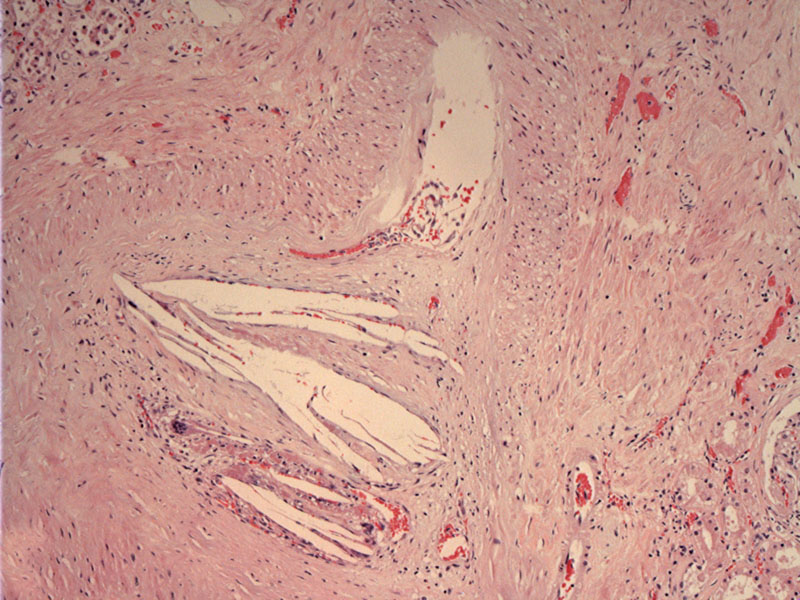
Vessel with cholesterol clefts -- the crystals themselves dissolve in the material used for histological processing, so needle-shaped spaces are seen on the slide.
){kind=link}
The cholesterol embolus results in ischemia distal to the vascular occlusion. There is the beginnings of an acute infarct, seen as coagulation necrosis. The tubules are losing their nuclear features and becoming ghost-like.
){kind=link}
Renal cholesterol crystal embolization, also known as atheroembolic renal disease, is due to showers of cholesterol crystals from an atherosclerotic aorta, resulting in occlusion of small renal arteries. Cholesterol crystal embolization can occur spontaneously or arise as a complication of an invasive vascular procedure such as aortic angiography. Sometimes, cholesterol emboli may occur following anticoagulant and fibrinolytic therapy. While the latter may seem counterintuitive, the mechanism of anticoagulation or fibrinolysis can disrupt complex plaques.
The early phase of this process involves fresh crystal emboli causing endothelial injury and an early histiocytic response. The intermediate phase involves a giant-cell reaction and intimal proliferation. The late phase consists of encasement of the crystals by histiocytes, more intimal proliferation, and fibrous tissue formation.
Usually affects elderly men with a history of diffuse atherosclerosis. Presentation may be acute with abrupt and sudden onset of renal failure or a progressive loss of renal function occurs over weeks. A third form of renal atheroemboli has been described, presenting as chronic, stable, and asymptomatic renal insufficiency.
No effective treatment exists. Anticoagulants should be avoided, while various antiplatelet drugs have been tried without success. Anecdotal reports suggesting that pentoxifylline may be beneficial exist but this remains unproven (Scolari).
Outcome is variable, resulting in different degrees of renal impairment. Some only have a moderate loss of renal function while others may succumb to severe renal failure requiring dialysis. In four reports, the 1-year mortality ranged from 64% to 87% (Scolari).
Cheng L, Bostwick DG, eds. Essentials of Anatomic Pathology. 2nd Ed. Totowa, NJ: Humana Press; 2006: 1142.
Scolari F,et al. Cholesterol crystal embolism: A recognizable cause of renal disease. Am J Kidney Dis. 2000 Dec;36(6):1089-109.