System: Mediastinum: Thymus: Neoplastic: Thymoma, B1 type

System: Mediastinum: Thymus: Neoplastic: Thymoma, B1 type

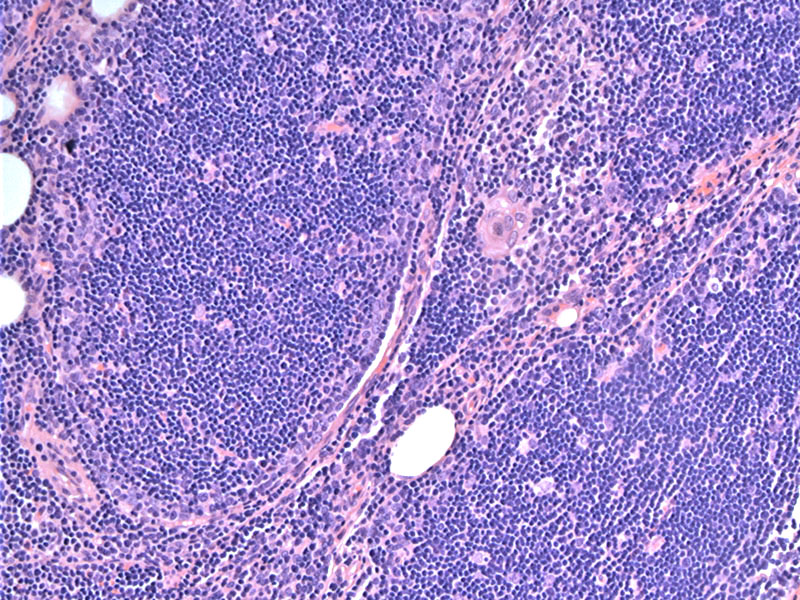
Type B1 resembles normal thymus, with lobules of lymphocytes.
Paler areas represent medullary differentiation, which are usually more discrete and circumscribed. Medullary differentiation represents foci of more mature T-cells (TdT negative).
Similar to the normal thymus cortex, it is rich in T lymphocytes, which are mostly immature (TdT positive). Epithelial cells are present, but it may require a cytokeratin stain to identify them in many areas.
Invasion into mediastinal fat renders this a stage II tumor. In large studies, the prognostic value of differentiating stages I from II appears clinically unimportant, as they showed no significant prognostic differences between the two groups.
CT scan of a B1 thymoma with mediastinal fat invasion (not apparent here) Image
the touch prep Image
gross with some invasion Image
low power Image
histo lots of lymphs Image
more Image
clinical staging Image
Type B1 thymoma resembles the normal functional thymus with well-formed lobules divided by fibrous septae. Among the type B thymomas, it contains the most numerous lymphocytes. Type B thymoma is considered the equivalent of the "lymphocyte‐rich" or "predominantly cortical thymoma" in the older classifications.
The epithelial cells are ovoid cells with round nuclei and small nucleoli, although some cells may be large and occasionally show conspicuous nucleoli. Unlike the other subtypes, the epithelial component does not form sheets or aggregates, rather, they are sparsely scattered throughout the background filled with lymphocytes. The lymphocytes are mostly immature T-cells (TdT positive) and there will be foci of paler areas representing medullary differentiation (composed of more mature T-cells that are TdT negative)(Fletcher).
Stage is the most important prognostic and predictive feature for the treatment of thymoma patients.
Meta-analysis indicates no statistically significant differences in survival rates among type A, AB, or B1 thymoma. Significant differences in survival rates between A/AB/B1 thymomas and B2 or B3 lesions are found, suggesting that the WHO classification of thymomas may be simplified into three categories. Survival for B1 is good, and on the order of 90%.
Type B1 thymoma consists of sheets and lobules of small round (cortical-like) thymic lymphocytes with single scattered thymic epithelial cells in the background
This thymoma best corresponds with lymphocyte-rich thymoma and the cortical or organoid thymoma in the MH system
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 1323-1327
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}