System: Endocrine: Thyroid: Neoplastic: CASTLE

System: Endocrine: Thyroid: Neoplastic: CASTLE

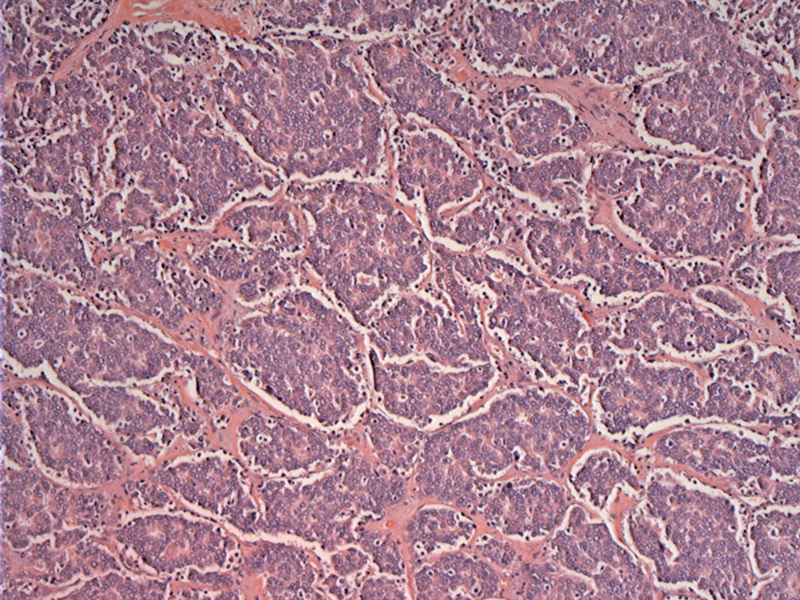
Case 1 - CASTLE shows a lobulated and expansive growth pattern, with fibrous septa dividing the tumor.
Distinct nests of tumor are separated by fibrous bands.
The neoplastic cells have large vesicular nuclei with prominent nucleoli. There is some pseudoacinar formation with a sprinkling of lymphocytes.
Crowded and overlapping nuclei are seen. The cells with moderate to little cytoplasm, some nuclear variation and finely dispersed chromatin.
IHC can differentiate CASTLE from other thyroid neoplasms. Similar to thymic carcinoma, CASTLE is positive for CD5, but the majority of thymomas or other malignancies are CD5-negative.
CASTLEs are immunoreactive for cytokeratin protein.
Expression of bcl-2 is diffusely positive. bcl-2 and mcl-1 are antiapoptosis proto-oncogenes reported to be expressed by the majority of true thymic carcinomas but only a minority of thymomas. Dorfman and colleagues examined cases of CASTLE compared to thymomas found increased expression of both bcl-2 CASTLE/thymic carcinomas (90%) compared to thymomas (33%). Similar percentages were found for mcl-1 (Dorfman).
Thyroglobulin is negative, as is TTF1. This helps to exclude some primary thyroid neoplasms.
FNA of this tumor shows a cellular aggregate of cells with a high N/C ratio and scant cytoplasm.
A closer look at the large dark cells -- some pleomorphism is seen. Of 27 FNAs performed on lesions later diagnosed as CASTLE, 23 cases were recognized as malignant cells, but only one case was signed out as CASTLE prior to the permanent section (Youens).
On the cell block - keratin 5 was positive and highlighted the neoplastic population.
Case 2 - This case has a much more spindled and microcystic appearance. Although this occurred in an adult, it may represent a case of SETTLE (see below for discussion of SETTLE).
Fibrous septations divide lobules of neoplastic cells.
Microcystic spaces were seen within the lesion.
The neoplastic cells have vesicular nuclei and prominent nucleoli.
These fascicles of spindle cells are quite different from the previous case in which the neoplastic cells are more plump and epithelioid.
The spindled areas merge into more tubulocystic or hemangiopericytoma-like pattern.
Carcinoma showing thymus-like differentiation (CASTLE) is a rare malignant neoplasm originally described by Miyauchi et al in 1985. It was described as an "intrathryoid thymoma" and is histologically indistinguishable from thymic carcinoma. It is thought to be derived from ectopic thymic remnants as a result of migration of thymic tissue derived from the third and fourth branchial during development (Youens).
CASTLE appears as a hard gray-tan mass in the lower pole of the thyroid. Lobules of tumor cells are separated by broad fibrous septae, reminiscent of a thymoma or thymic carcinoma (Fletcher). The tumor cells often have vesicular nuclei with prominent nucleoli, with indistinct cell borders. Occasionally, they can assume a more squamoid or spindled appearance. Varying numbers of lymphocytes infiltrate the septae and tumor cells (Fletcher).
In terms of IHC, the neoplastic cells are positive for CD5, CD117, CEA, p63 and high molecular weight keratins, an immunoprofile shared by thymic carcinomas. They are not reactive for thyroglobulin, calcitonin and TTF-1 (Fletcher, Youens).
The differential diagnosis of CASTLE includes undifferentiated thyroid carcinoma and squamous cell carcinoma of the thyroid. As CASTLE has much better prognosis, it is important to make this distinction (Youens). Fortunately, the immunoprofile described above is not seen in entities other than thymic carcinomas and CASTLE.
A note on CASTLE and SETTLE:
Chan and Rosai (1991) divided tumors of the neck arising from ectopic thymic remnants into four categories: (1) ectopic hamartomatous thymoma, (2) ectopic cervical thymoma, (3) spindle epithelial tumor with thymus-like differentiation (SETTLE), (4) and CASTLE.
SETTLE stands for spindle epithelial tumor with thymus-like differentiation. Whereas CASTLE tends to arise in older adults, SETTLE affects children and adolescents, although cases of SETTLE have been reported in adults.
Histologically, SETTLE is composed of spindle cells that form fascicles. Neoplastic cells also form tubulocystic structures, papillae and tubules. In some instances, the cysts and glands are lined by mucinous or even respiratory epithelium (Nisa). Unfortunately, characterization of SETTLE and prognosis of SETTLE is lacking due to the rarity of the condition. Only about 25 cases have been described in the literature thus far. However, it seems like SETTLE also shows indolent growth, but with a tendency to develop delayed metastases (Nisa, Grushka).
Affects older adults (mean age of 48) and presents with a thyroid mass. In a third of cases, there is metastasis in the regional lymph nodes at the time of diagnosis.
Median sternotomy is an excellent approach, and complete resection is important. CASTLE with lymph node involvement has a high risk of recurrence when treated by surgery and radiotherapy. Surgery alone is possible for tumors without lymph node metastasis.
Relatively good prognosis with indolent behavior. Delayed local recurrence is common, but most have long survivals after surgery with adjuvant radiation.
→CASTLE arise from ectopic thymic remnants.
→Immunoprofile and histology are identical to thymic carcinomas.
Dorfman DM, Shahsafaei A, Miyauchi A. Immunohistochemical staining for bcl-2 and mcl-1 in intrathyroidal epithelial thymoma (ITET)/carcinoma showing thymus-like differentiation (CASTLE) and cervical thymic carcinoma. Mod Pathol. 1998 Oct;11(10):989-94.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 1048.
Grushka JR, Ryckman J, Mueller C et al. Spindle epithelial tumor with thymus-like elements of the thyroid: a multi-institutional case series and review of the literature. J Pediatr Surg. 2009 May;44(5):944-8.
Nisa A, Barakzai A, Minhas K, Kayani N. Spindle epithelial tumor with thymus-like differentiation of thyroid gland: Report of two cases with follow-up. Indian J Pathol Microbiol 2010;53:781-4
Reimann JD, Dorfman DM, Nosé V. Carcinoma showing thymus-like differentiation of the thyroid (CASTLE): a comparative study: evidence of thymic differentiation and solid cell nest origin. Am J Surg Pathol. 2006 Aug;30(8):994-1001.
Youens KE, Bean SM, Dodd LG, Jones CK. Thyroid carcinoma showing thymus-like differentiation (CASTLE): Case report with cytomorphology and review of the literature. Diagn Cytopathol. 2011 Mar;39(3):204-9.
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}