
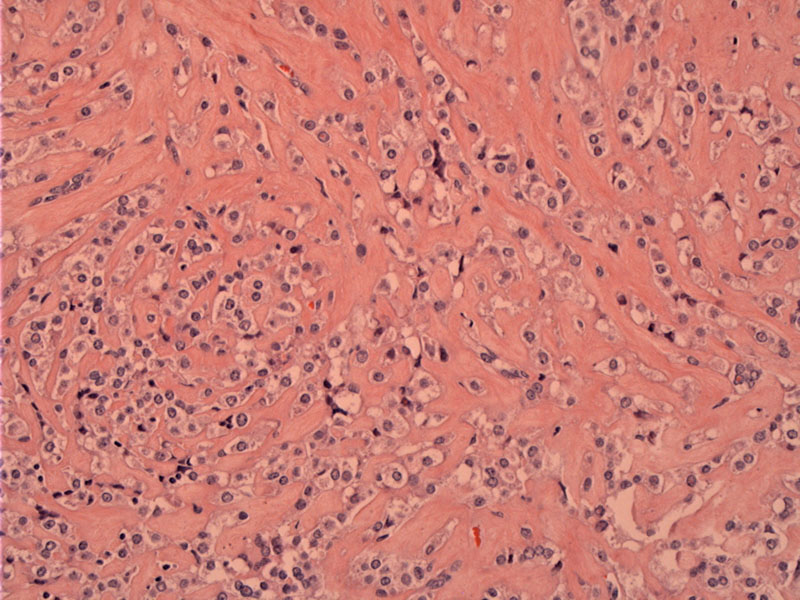
PEComas can grow in a variety of patterns including a growth pattern, or arranged in fascicular bundles or diffuse sheets. A network of small capillaries distributed throughout the tumor has been described in most instanced. Varying degrees of stromal hyalinization, as seen here, represents another recognized feature.
){kind=link}
The lesion-myometrial interface shows a circumscribed lesion that irregularly admixes with the normal smooth muscle cells.
){kind=link}
Cells show a fair amount of clear cytoplasm and rounded cellular outlines, yielding a distinctly epithelioid appearance.
){kind=link}
The uterus and retroperitoneum are the most frequently involved sites of perivascular epithelioid cell tumors (PEComas). This neoplasm remains poorly defined, characterized by spindle and epithelioid cells with clear to eosinophilic cytoplasm that have immunoreactivity for melanocytic markers, most frequently HMB-45. They also demonstrate a highly characteristic network of small capillaries reminiscent of clear cell RCC. PEComas have also been described in the cervix, vagina, pelvis, broad ligament, and ovary (Fadare) and arise predominantly in females.
In the uterus, there is the possibility of diagnostic confusion with epithelioid smooth muscle tumors. There is significant clinicopathologic overlap between these two entities. While PEComas demonstrate immunoreactivity for melanocytic markers by definition, these markers may be focally positive in epithelioid smooth muscle tumors. Desmin and smooth muscle actin, IHC stains that usually support the diagnosis of leiomyomas (smooth muscle tumors), may also be positive in a significant number of PEComas. Therefore, reliance on morphology is of importance.
Fadare in the 2008 article published in Int Seminars in Surgical Oncology (referenced below), provides a detailed discussion on how to distinguish between epithelioid smooth muscle tumors and PEComas. He elegantly summarizes the difference as such "In the simplest analysis of the overlap, smooth muscle neoplasia may be viewed as uterine tumors that always display myomatous differentiation and occasionally display melanocytic differentiation, whereas PEComas always display melanocytic differentiation and usually displays some myomatous differentiation."
PEComas are not sufficiently homogeneous to allow for a uniform statement about their prognosis, as they seem to represent a group of tumors with a range of behaviors. (Fadare). Larger tumors and those with coagulative necrosis, significant cytologic atypia, or high mitotic counts are more likely to behave in a malignant fashion compared to smaller ones (Fadare). However, beware, as rare cases showing very minimal to no mitotic activity have shown metastatic behavior!
In a study of 35 PEComas from a variety of sites, Folpe prognostically classified them into 3 groups: (1) a malignant group comprised of tumors with 2 or more worrisome features (>5 cm, infiltrativeness, high nuclear grade and cellularity, mitotic rate >=1/50 HPF, necrosis, and LVI), (2) a benign group that lacks all of the aforementioned features, and (3) a group of tumors of “uncertain malignant potential” characterized by tumors >5 cm in size OR nuclear pleomorphism/giant cells as the only worrisome feature. It is not clear, however, if this system is directly applicable to uterine PEComas.
• Lung : Lymphangioleiomyomatosis
• Myometrium : Leiomyosarcoma, Epithelioid Variant
Fadare O. Uterine PEComa: appraisal of a controversial and increasingly reported mesenchymal neoplasm. Int Semin Surg Oncol. 2008 Mar 6;5:7.
Fadare O. Perivascular epithelioid cell tumor (PEComa) of the uterus: an outcome-based clinicopathologic analysis of 41 reported cases. Adv Anat Pathol. 2008 Mar;15(2):63-75.
Folpe AL, Mentzel T, Lehr HA, et al. Perivascular epithelioid cell neoplasms of soft tissue and gynecologic origin: a clinicopathologic study of 26 cases and review of the literature. Am J Surg Pathol. 2005;29:1558–1575