
Embryonal carcinoma is seen in this mixed GCT, consisting of anaplastic cells with indistinct cell borders. Note the foci of necrosis.
){kind=link}
Mesenchymal stroma is seen merging with embryonal carcinoma (upper left). The stroma can range from relatively acellular and sometimes slightly hyalinized to more typically densely cellular regions. The presence of cellular mesenchyme on its own does not warrant a designation of teratoma.
){kind=link}
CD30 (Ki-1) highlights the membranes of neoplastic embryonal carcinoma cells.
){kind=link}
Another image of embryonal carcinoma -- note that the tumor cells are larger than those in seminoma and yolk sac tumor, with more hyperchromatic irregular nuclei.
){kind=link}
Choriocarcinoma is especially prone to present with metastases rather than forming a discrete mass. See a plexiform arrangement of syncytiotrophoblast cells with mononucleated, mostly cytotrophoblast cells around foci of hemorrhage.
){kind=link}
Another image of choriocarcinoma, with syncytiotrophoblastic giant cells overlying cytotrophoblasts. Note the surrounding hemorrhage, a very common feature in choriocarcinomas.
){kind=link}
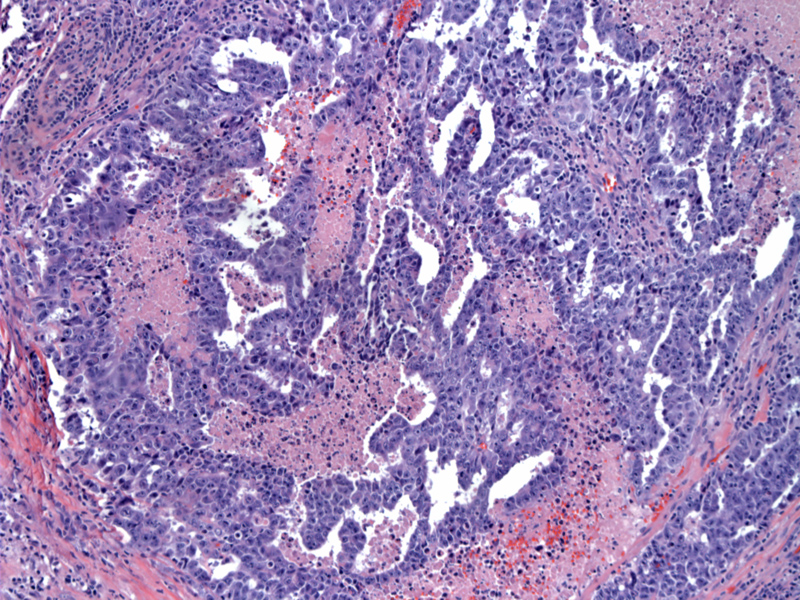
This image demonstrates a yolk sac tumor area - a common component of mixed germ cell tumors of the testis. Note the hyaline globules and loose microcystic architecture typical of YST.
){kind=link}
AFP highlights yolk sac tumor areas. Note the Schiller-Duval body in the upper image.
){kind=link}
Most teratomatous elements in the testis occur as a component of mixed germ cell tumors, which represent about one-third of germ cell tumors and contain teratoma in about half of the cases (Ulbright).
){kind=link}
Approximately 40% of testicular tumors are 'pure' with a single histologic pattern while the remaining 60% are mixed, with a combination of two or more histologic types. The most common combinations include:1
- Teratoma and embyronal carcinoma (25%)
- Embryonal carcinoma and seminoma (15%)
- Teratoma, embryonal carcinoma, seminoma (15%)
- Seminoma and yolk sac tumor (<1%)
- Yolk sac tumor is identified in up to 40% of MGCTs
Not surprisingly, MGCTs have a variegated gross appearance which reflects its motley composition, with a mixture of cystic and solid areas. Although one must examine the tumor microscopically, necrosis and hemorrhage suggest the presence of embryonal carcinoma and/or choriocarcinoma. Bony, cartilaginous or sebaceous areas suggest teratomatous elements.1
IHC will be helpful in identifying the different components. AFP will highlight yolk sac tumor, hCG will highlight syncytiotrophoblasts in choriocarcinomas and Ki-1 (CD30) is positive in embryonal carcinomas. PLAP is focally positive in all GCTs.1
Age at diagnosis is usually between 30s and 40s. Presents as painless testicular enlargement, but in advanced disease, patients may present with symptoms due to metastasis such as hemoptysis (lung involvement).1,2
It is important to carefully describe the various histologic subtypes and their contribution to the overall tumor, as this influences treatment decisions. Nonseminomatous GCTs are treated differently than seminomas, and increased percentages of embryonal carcinoma and choriocarcinoma worsens prognosis and warrants more aggressive therapy.
Adverse prognostic factors include advanced stage tumors, greater proportion of embryonal carcinoma and choriocarcinoma, and presence of angiolymphatic invasion.2
• Testis : Pure Yolk Sac Tumor
• Testis : Seminoma, Classic Type
• Testis : Embryonal Carcinoma
1 Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 829-830.
2 Zhou M, Magi-Galluzzi, C. Genitourinary Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elvesier; 2006: 568-70.
Ulbright TM. Germ cell tumors of the gonads: a selective review emphasizing problems in differential diagnosis, newly appreciated, and controversial issues Modern Pathology (2005) 18, S61–S79.