
Thickened mucosal basement membrane and edema in the lamina propria are seen. Dilated lymphovascular channels, if prominent, are sometimes subclassifed as pseudoangiomatous sinonasal polyps but in fact these areas are just foci of edema.
){kind=link}
Note the pale color of the lamina propria due to expansion from fluid. Scattered chronic inflammatory cells can be seen.
){kind=link}
Markedly edematous stroma throws the surface into polypoid configuration. Again, a pseudoangiomatous pattern can be seen.
){kind=link}
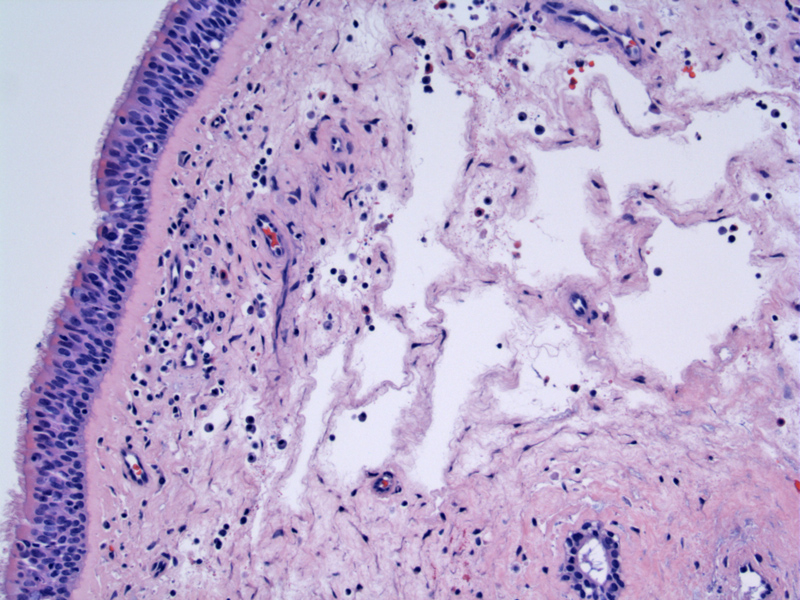
Another image of edema in the lamina propria with relatively scant inflammation.
){kind=link}
An admixture of eosinophils and lymphocytes are present in the stroma. If polyps are due to an allergic etiology, a prominent population of eosinophils may be present.
){kind=link}
In this allergic polyp, there is also basement membrane thickening underlying a normal respiratory mucosa.
){kind=link}
Stromal edema is prominent (asterix) as are numerous eosinophils and lymphocytes.
){kind=link}
Common associations with sinonasal polyps include chronic rhinosinusitis, allergy, asthma, vasomotor rhinitis, cystic fibrosis and aspirin hypersensitivity. Although the exact etiology of sinonasal polyps is unknown, it is most likely related to a chronic underlying inflammatory condition such as is seen in cystic fibrosis and asthma. A multitude of cytokines and antibodies have been investigated as inflammatory mediators in polyp formation. Patients with nasal polyps secondary to asthma are often found to have more severe asthma than patients without polyps, furthering a systemic inflammatory mediator hypothesis.
Grossly, sinonasal polyps are pale, glistening and translucent. In contrast, antrochoanal polyps are firmer and not translucent. Microscopically, conventional sinonasal polyps consist of a loose edematous stroma with chronic inflammation (Thompson).
There is no racial or sex predilection to polyp formation. Patients often present with nasal congestion, hyposmia (reduced ability to smell), headache and facial pain.
Sinonasal polyposis is uncommon in children, but when seen in this population, is often associated with cystic fibrosis. Up to 20% of children with CF have nasal polyps.
Sinonasal polyps are also associated with asthma -- approximately 30% of asthma patients have sinonasal polyps. Of note, Sampter's triad consists of bronchial asthma, nasal polyps and aspirin intolerance (Thompson).
Management options include topical and oral steroids, antibiotics, diuretic nasal washes, intrapolyp injection of steroids, polypectomy, and functional endoscopic sinus surgery.
Sinus polypectomy can result in a marked reduction of polyps with a consequent improvement in quality of life, however, despite surgical removal, polyps recur in the majority of affected individuals (Poetker).
• Sinonasal : Antrochoanal Polyp
Poetker DM, Mendolia-Loffredo S, Smith TL. Outcomes of endoscopic sinus surgery for chronic rhinosinusitis associated with sinonasal polyposis. Am J Rhinol. 2007 Jan-Feb;21(1):84-8.
Thompson LDR. Endocrine Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier; 2006: 89-93.