
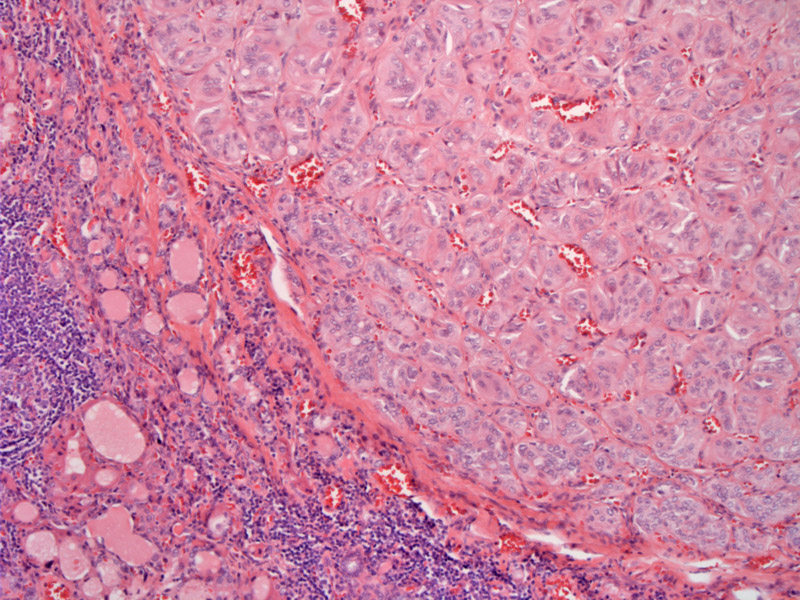
The lesion presents as a well demarcated small lesion, composed of medium sized polygonal or slightly elongated cells. There is no actual capsule.
){kind=link}
Polygonal cells arranged in a trabecular architecture are present throughout the lesion. The cells contain weakly eosinophilic cytoplasm and there is a limited stromal presence.
){kind=link}
Some nuclear irregularities including focal clearing and grooves are typical.
){kind=link}
Intranuclear inclusions can even be identified, a problem for the cytopathologist and possibly upon resection. Hyalinized stroma surround the trabeculae.
){kind=link}
Hyalinizing trabecular adenoma was thought to be a variant of papillary carcinoma upon discovery of RET/PTC mutations (Cheung). However, due to their seemingly benign behavior, many were unwilling to accept this idea. A study of their behavior in 118 cases proved that the all tumors were noninvasive, nonrecurring, and nonmetastasizing neoplasms (Carney, Dec 2008). Therefore, the designation hyalinizing trabecular adenoma seems to be appropriate for them.
Histologically, the neoplastic cells can be polygonal or spindled, and are arranged in broad trabeculae. A variably hyalinized stroma surrounds the trabeculae. It is important to recognize this entity as it can often be misdiagnosed as papillary carcinoma on FNA or as papillary or medullary carcinoma on H&E.
Medullary carcinoma should be positive for calcitonin and neuroendocrine markers, whereas these markers are usually absent or only focally positive in HTA. Interestingly, the hyaline material surrounding the tumor trabeculae (amyloid in the case of mecullary carcinoma) may both stain with Congo red and amyloid markers, and thus, these stains may not be helpful in distinguishing between the two entities (Evenson).
HTA may demonstrate nuclear features of papillary thyroid carcinoma as well as the presence of RET/PTC1. However, HTA do not exhibit RAS or BRAF mutations. Strong peripheral cytoplasmic and membranous staining of the neoplastic cells with MIB-1 immunostain is fairly unique to HTA and may be helpful if it is available at your institutation (Nose).
Wide age range, described from between 21 and 79 years of age (Carney, Dec 2008).
Excellent. Only rare cases have been reported to be malignant, thus, HTA should be thought of as a lesion with low malignant potential (Nose).
→Hyalinizing trabecular carcinoma used to be considered a variant of papillary thyroid carcinoma because HTC can exhibit nuclear features of PTC as well as the RET/PTC1 translocation.
→It is now considered a separate entity with very low malignant potential, justifying the designation of adenoma.
→Key differential diagnostic considerations are medullary carcinoma and papillary thyroid carcinoma.
• Thyroid : Papillary Thyroid Carcinoma
• Thyroid : Medullary Carcinoma
Carney JA, Hirokawa M, Lloyd RV, Papotti M, Sebo TJ. Hyalinizing trabecular tumors of the thyroid gland are almost all benign. Am J Surg Pathol. 2008 Dec;32(12):1877-89.
Carney JA. Hyalinizing trabecular tumors of the thyroid gland: quadruply described but not by the discoverer. Am J Surg Pathol. 2008 Apr;32(4):622-34.
Cheung CC, Boerner SL, MacMillan CM, et al. Hyalinizing trabecular tumor of the thyroid: a variant of papillary carcinoma proven by molecular genetics. Am J Surg Pathol. 2000;24:1622–1626.
Evenson A, Mowschenson P, Wang H et al. Hyalinizing trabecular adenoma--an uncommon thyroid tumor frequently misdiagnosed as papillary or medullary thyroid carcinoma. Am J Surg. 2007 Jun;193(6):707-12.
Nosé V, Volante M, Papotti M. Hyalinizing trabecular tumor of the thyroid: an update. Endocr Pathol. 2008 Spring;19(1):1-8.