
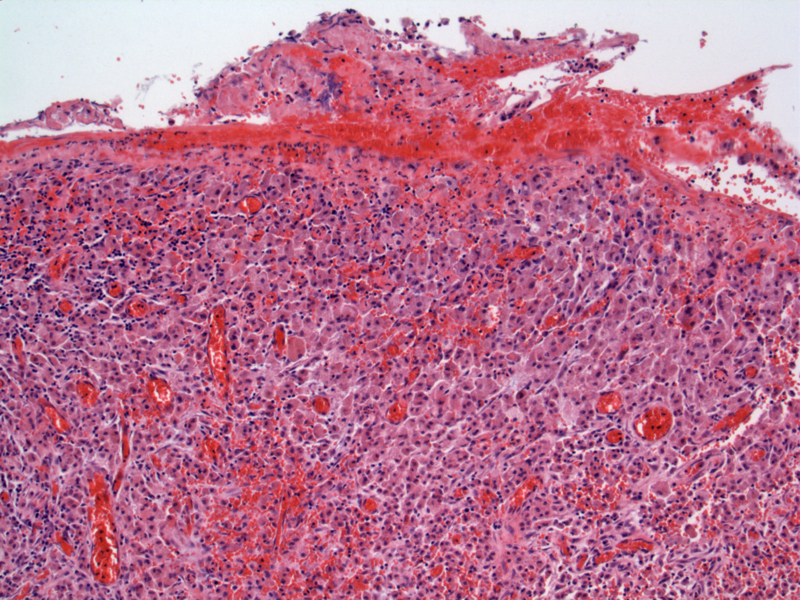
The gallbladder surface is eroded and there is secondary hemorrhage. Mucosal ulceration and bile extravasation are thought to be the underlying cause of this unusual process.
){kind=link}
Irregular dense fibrosis alternates with confluent areas of mixed chronic inflammation with a histiocytic predominance.
){kind=link}
The inflammatory process is exuberant, and may even infiltrate out into the surrounding adipose tissue. Xanthogranulomatous cholecystitis can not only be infiltrative but also destructive locally.
){kind=link}
Among the xanthomatous cells are scattered multinucleated giant cells in various numbers.
){kind=link}
Xanthogranulomatous cholecystitis starts as an acute inflammatory process followed by a granulomatous reaction and then a cellular-type immunologic response. In such ways, it resembles xanthogranulomatous pyelonephritis, in which chronic infection and calculi are common findings.
Average age is mid 50s. In about 15% of cases, the radiological impression is suspicious for carcinoma. The relation to cholelithiasis is high, from 95% to 100%.
Firm adhesions of the gallbladder to adjacent tissues are common and lead to difficulty in surgical treatments. As such, there is a relatively high rate of conversion from laparoscopic to open cholecystectomy.
• Gallbladder : Follicular Cholecystitis
• Gallbladder : Choledocholithiasis
• Kidney : Xanthogranulomatous Pyelonephritis
Yang T, Zhang BH, Zhang J, Zhang YJ, Jiang XQ, Wu MC. Surgical treatment of xanthogranulomatous cholecystitis: experience in 33 cases. Hepatobiliary Pancreat Dis Int. 2007 Oct;6(5):504-8.