System: Head and Neck: Larynx: Pre-Neoplastic: Recurrent Laryngeal Papillomatosis

System: Head and Neck: Larynx: Pre-Neoplastic: Recurrent Laryngeal Papillomatosis

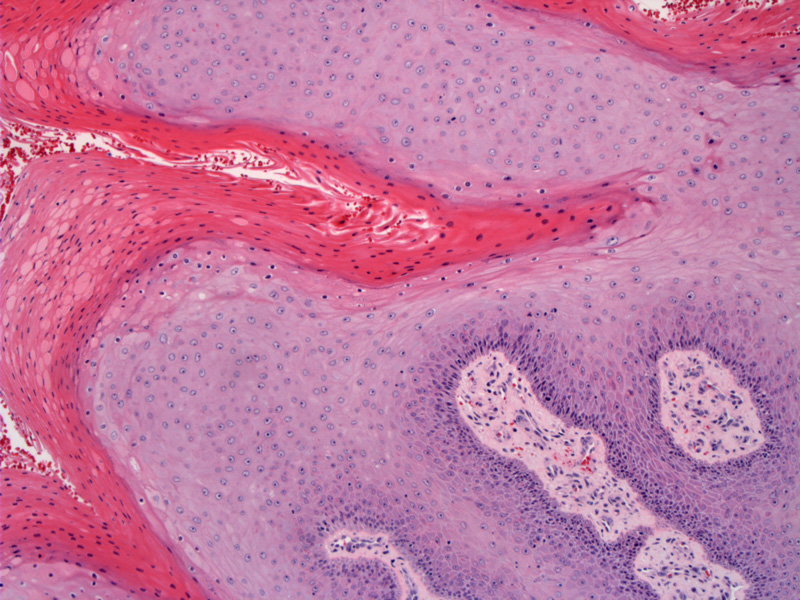
Case 1: Papillary squamous proliferation with abundant parakeratosis.
Often abundant keratin is associated with these lesions.
The lesion may show atypia at base due to inflammation and frequent debridement.
Recurrent laryngeal papillomatosis, also known as recurrent respiratory papillomatosis (RRP), demonstrates a bimodal distribution: juvenile onset and adult onset. Juvenile-onset recurrent respiratory papillomatosis (JORRP) occurs in children younger than 5 years. The second age peak, known as adult-onset recurrent respiratory papillomatosis (AORRP), occurs between the ages of 20 and 40 years old with a mode of transmission thought to be either latent virus present from birth or adult exposure through sexual contact (Gallagher). The younger the patient's age at diagnosis, the more likely the patient will have severe disease (Leung).
Human papilloma virus (HPV) has been implicated as the etiologic agent of RRP. RRP is almost universally caused by HPV types 6 and 11, the same types that cause genital warts. HPV type 11 is more likely to cause severe disease and is associated with earlier presentation. It tends to require more frequent debridement, has a higher risk of bronchopulmonary spread, and more often requires tracheotomy (Wiatrak).
Currently, there are no medical or surgical cures. Goals include eradication of disease from the airway, improvement in voice quality, and control of disease spread. Surgical management remains the fundamental therapy.
The most commonly utilized medical therapy is intralesional cidofovir (Vistide, Pharmacia & Upjohn, Erlangen, Germany) (Pransky). Cidofovir is a nucleoside analog of deoxycytidine monophosphate that once converted into its active form, becomes incorporated into DNA and is toxic against the herpesvirus family.
RRP has an unpredictable course and tend to recur and/or spread throughout the respiratory truct. Complications include stenosis and a small risk of progression to dysplasia/carcinoma.
Gallagher TQ, Derkay CS. Recurrent respiratory papillomatosis: update 2008. Curr Opin Otolaryngol Head Neck Surg. 2008 Dec;16(6):536-42
Leung R, Hawkes M, Campisi P. Severity of juvenile onset recurrent respiratory papillomatosis is not associated with socioeconomic status in a setting of universal healthcare. Int J Pediatr Otorhinolaryngol 2007; 71:965–972.
Wiatrak DW, Broker TR, Lewis L. Recurrent respiratory papillomatosis: a longitudinal study comparing severity associated with human papilloma viral types 6 and 11 and other risk factors in a large pediatric population. Laryngoscope 2004; 114(Suppl 104):1–23.
Pransky SM, Albright JT, Magit AE. Long-term follow-up of pediatric recurrent respiratory papillomatosis managed with intralesional cidofovir. Laryngoscope 2003; 113:1583–1587.

){kind=link}
){kind=link}
){kind=link}