
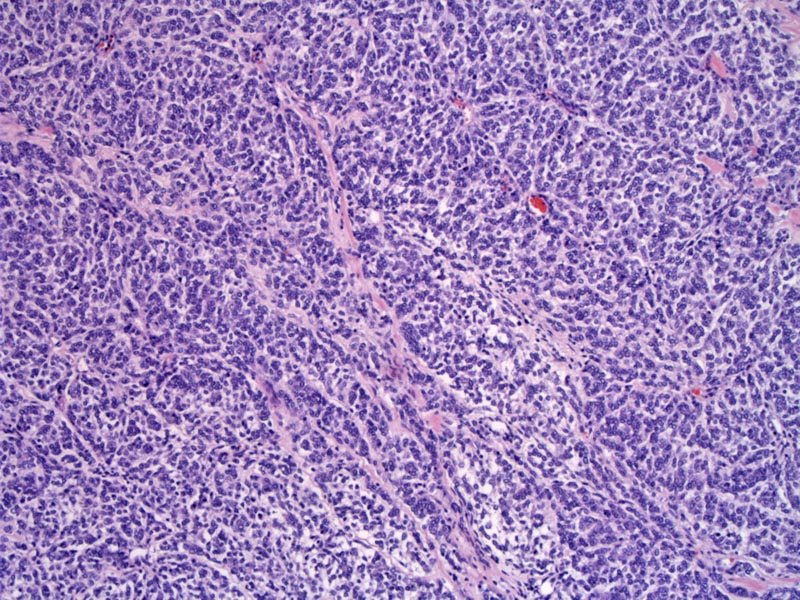
There is a monotonous sheet of cells with pale staining cytoplasm. Unlike clear cell renal cell carcinoma, the cytoplasm is not really clear. There is a background of small delicate branching vessels, and if one can find the tumor interface, there should be an infiltrative border between the sarcoma and the normal parenchyma.
){kind=link}
The vesicular nuclei contain finely dispersed chromatin with inconspicuous nucleoli. Note the mitotic figure in the center. Mitosis can be seen, but not as frequently as in Wilms tumor.
){kind=link}
Previously known as "bone-metastasizing renal tumor of childhood", clear cell sarcomas are malignant pediatric tumors that tend to metastasize to the bones. In fact, these tumors are 10x more likely to metastasize to the bone compared to other pediatric kidney tumors (Fletcher). Note that clear cell sarcoma of the kidney bear NO relationship to clear cell sarcoma of the soft tissues -- they are completely different tumors. Clear cell sarcoma of soft parts resemble melanomas and have a characteristic t(12;22) translocation, not seen in clear cell sarcoma of the kidney.
Grossly, these tumors are unilateral, solitary, irregularly shaped with a homogeneous grey-tan cut surface. Cystic changes can be seen. The tumor can be large, weighing over 500 grams.
In contrast to Wilms tumor (the main differential), there are no blastema elements and mesenchymal elements such as cartilage or muscle. The vascular pattern characteristic of clear cell sarcoma is not seen in Wilms tumor. Grossly, Wilms tumor tend to be multicentric and bilateral whereas clear cell sarcomas are unicentric and unilateral. IHC may be very helpful as clear cell sarcomas only stain with vimentin and are negative for most other markers such as WT1 (Fletcher, Zhou).
Most patients are between 12-36 months of age (close to the same age range as Wilms tumors). Clear cell sarcomas are rare in adulthood. 2/3 of patients are males.
It is important to distinguish clear cell sarcomas from Wilms tumors because the treatment is very different. Clear cell sarcomas do not respond to the chemotherapy used for Wilms tumors, but can respond to doxorubicin regiments (Fletcher).
Nephrectomy followed by doxorubicin regimen has improved survival rates. Late relapses tend to present as bone metastases (Zhou).
→This tumor likes to metastasis to the bone.
→Polygonal cells with deceptively bland nuclei are arranged in nests; a network of arcuate blood vessels can be seen in the background.
→Don't confuse clear cell sarcoma of kidney with clear cell sarcoma of soft parts. They are completely different tumors.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 515-6.
Zhou M, Magi-Galluzzi, C. Genitourinary Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elvesier; 2006: 317-9.