
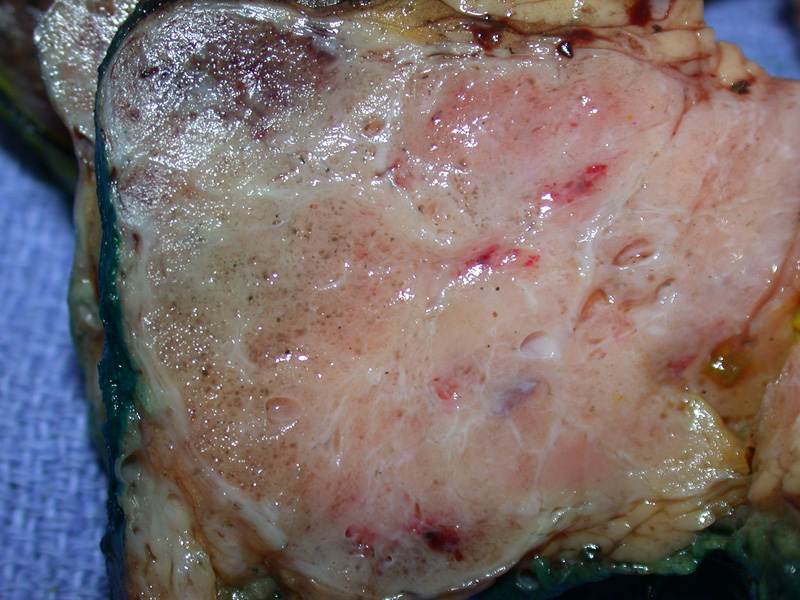
The tumor is a well-circumscribed round lesion with a cut surface showing tiny cysts with a few larger cysts and radiating bands of white fibrosis. The edges of the tumor are a bit lobulated, but the junction with the adjacent pancreas is discrete. Although not obvious in this image, a central stellate scar is characteristic.
){kind=link}
The neoplasm consists of a proliferation of microglandular cysts lined by attenuated epithelial cells separated by fibrocollagenous stroma. Small intraluminal papillary projections may also be seen.
){kind=link}
The lesional cysts push into normal pancreas, with no demarcated capsule.
.', 'micro', '')){kind=link}
Cyst size varies, with smaller ones interspersed among larger ones. Pale staining acellular serous fluid is seen in some lumens.
){kind=link}
Some cystic structures appear back to back, and areas of fibrotic stroma are also present. Note that the epithelial cells are usually described as cuboidal with clear glycogen-rich cytoplasm. However, due to processing and pressure of cystic fluid, the epithelial cells may be more attenuated and eosinophilic.
){kind=link}
Some cysts have scant hyalinzed fibrotic stroma between them, leading to the impression of a swiss cheese appearance.
){kind=link}
Serous cystic neoplasms include the following entities: serous microcystic adenoma, serous oligocystic and ill-demarcated adenoma (SOIA, macrocystic serous cystadneoma), von Hippel-Lindau associated cystic neoplasms (VHL-CNs), solid cystic adenoma and serous cystadenocarcinoma (Fletcher). The latter two entities are so rare that I will not discuss them.
All these entities have the following in common: the cysts are lined by glycogen-rich (PAS-positive) epithelial cells which exhibit a ductal immunoprofile (Fletcher). These cells may form micropapillary structures (Iacobuzio-Donahue, JHPCW). However, there are clinicopathologic differences between these serous cystic neoplasms. For serous microcystic adenomas, they tend to be located in the body or tail of the pancreas and almost all occur in women. However, in SOIAs (which exhibit larger cysts, hence their alternative designation "macrocystic serous cystadenoma") are usually located in the head of the pancreas and have equal gender predilection. Additional, VHL-CNs arise in multiple areas of the pancreas and can merge to involve the entire organ. As with SOIA, VHL-CNs patients are both males and females (Fletcher).
These differences are corroborated molecularly with VHL-CNs exhibiting both LOH at chromosome 3p (containing the VHL gene) AND germ line mutation of the VHL gene. In contrast, one study (Moore 2001) of 21 serous microcystic adenomas found that 50% exhibited LOH at 10q. In another study (Kim 2003), approximately 56% (8/14) exhibited LOH at 3p.
Grossly, serous microcystic adenomas can be large (range of 2.5 to 16cm) and are solitary. Again, multifocal masses may be associated with Von Hippel-Lindau syndrome. There is a honeycomb appearance with a central stellate scar. Histologically, the cysts are lined by cuboidal cells with clear cytoplasm; hyalinized fibrous tissue is seen between the cysts (Fletcher, JHPCW).
Serous microcystic adenomas usually arises in older individuals, occurring in the 6th decade, with a marked female preponderance. Presentation may be incidental (1/3 of cases), or symptomatic with abdominal pain and an enlarging mass. In SOIAs and VHL-CNs, there is no female predilection.
Benign tumors with excellent prognosis.
→Benign lesion consisting of epithelial-lined serous cysts.
→Predilection toward women in their 60s.
→When multifocal, think about Von Hippel-Lindau syndrome.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 474-6.
John Hopkins Pancreas Cancer Web (JHPCW). Available at http://pathology2.jhu.edu/pancreascyst/testcysts.cfm Accessed on Sept 4th, 2010.
Kim SG, et al. Comparison of epigenetic and genetic alterations in mucinous cystic neoplasm and serous microcystic adenoma of pancreas. Mod Pathol. 2003 Nov;16(11):1086-94.
Iacobuzio-Donahue CA, Montgomery EA. Gastrointestinal and Liver Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier; 2005: 484-5.
Moore PS, et al. Molecular characterization of pancreatic serous microcystic adenomas: evidence for a tumor suppressor gene on chromosome 10q. Am J Pathol. 2001 Jan;158(1):317-21.