
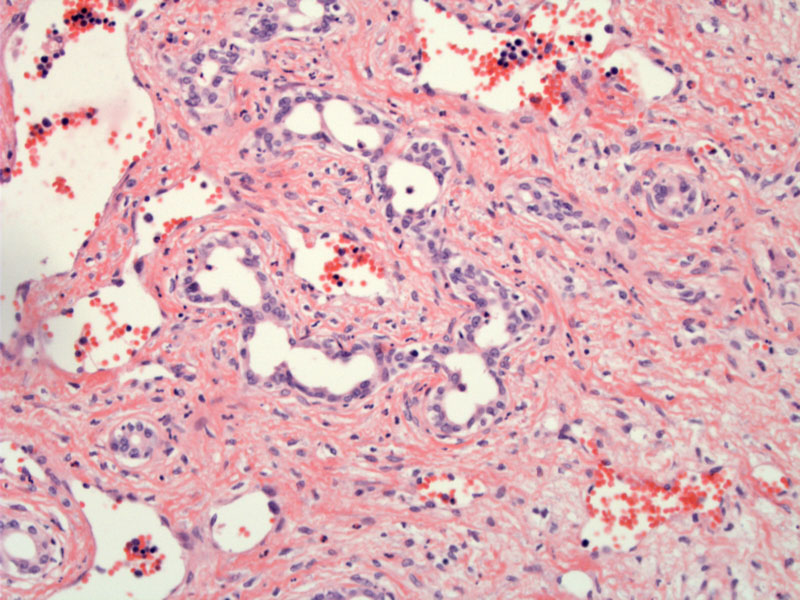
Vascular channels are lined by prominent, plump endothelial cells.
A proliferation of vascular channels can be appreciated, separated by a loose stroma.
The most common types of benign liver tumors in children are hemangiomas (of which infantile hemangioendothelioma is a subtype) followed by focal nodula hyperplasia, whereas the most common malignant tumors are hepatoblastoma and hepatocellular carcinoma (Gow).
Infantile hemangioendothelioma (IHE) may be solitary or multicentric and multinodular. They appear red, soft and spongy due to their vascularity. Microscopically, there is a proliferation of vascular channels lined by prominent endothelial cells and separated by a loose, sometimes edematous stroma. Portal tracts may be entrapped within the tumor (Iacobuzio).
Most patients are less than 6 months old, and there is a slight female predilection (M:F of 1:2). Typical presentation includes an abdominal mass and 10% have cutaneous hemangiomas. In up to 50% of patients, there is high output cardiac failure as a result of A-V shunting of the tumor (Gow, Cheng).
Plalelet sequestration within the tumor may lead to thromocytopenia and bleeding, known as Kasabach-Merritt syndrome (Gow, Iacabuzio). There is an association with other congenital anomalies, such as bilateral renal agenesis, Beckwith-Wiedemann syndrom, and mengomyelocele. Serum AFP levels are usually within the normal range.
Tumors may regress but most often patients undergo resection, embolization, or other treatment. Corticosteroids and supportive care including diuretics and blood product replacement (for coagulopathy) have been employed.
Usually regresses in the first two years of life, however, if consumptive coagulopathy and platelet sequestration occurs, there may be life-threatening hemorrhage. Also, if high-output cardiac failure ensues, treatment is indicated.
Almost always arises in children under 6 months
Although benign these tumors may cause cardiac or hepatic failure, requiring intervention
Cheng L, Bostwick DG, eds. Essentials of Anatomic Pathology. 2nd Ed. Totowa, NJ: Humana Press; 2006: 1425.
Gow KW, Bennett OL. Liver Tumors in Pediatrics: eMedicine.
http://emedicine.medscape.com/article/940516-overview
Last accessed on Sept 11, 2010.
Iacobuzio-Donahue CA, Montgomery EA. Gastrointestinal and Liver Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier; 2005: 613-5.

){kind=link}
){kind=link}