
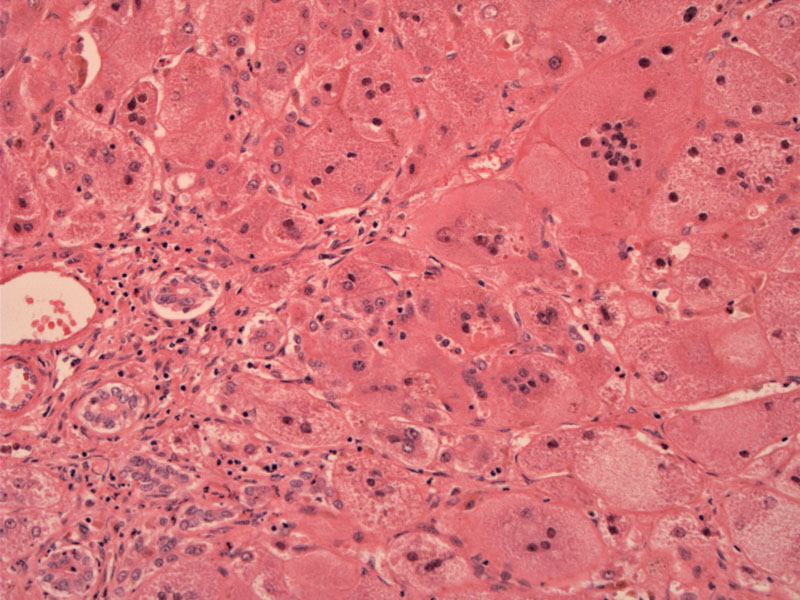
The fusion of several hepatocytes to form syncytial giant cells is a striking feature. Note the architectural disarray of the lobules.
){kind=link}
Some chronic inflammation and pericellular fibrosis can be seen the lobules.
){kind=link}
Neonatal giant cell hepatitis, also known as syncytial giant cell hepatitis, is a frequent pattern of neonatal liver injury, primarily seen in the first three months of life. It is important to distinguish this from biliary atresia which is treated surgically. Rare cases have been reported in adults (post-infantile giant cell hepatitis) in what is presumably autoimmune hepatitis.
Neonatal giant cell hepatitis likely represents a non-specific response to liver injury caused by infection, autoimmune disease, cholestasis, drugs, neoplasia, or metabolic disease. A commonly associated disorder is alpha-1-antitrypsin deficiency (Cheng).
Microscopically, one sees lobular disarray, cholestasis and most strikingly, syncytial giant cell transformation of hepatocytes via cell fusion or inhibition of mitoses. Note that the bile ducts are normal whereas ductular proliferation is seen in extrahepatic biliary atresia.
Patients present with jaundice, failure to thrive and hepatosplenomegaly. These symptoms similar to extrahepatic biliary atresia, and thus, must be distinguished by laboratory findings, imaging and biopsy.
Treatment depends on underlying condition.
Associated with alpha-1 antitrypsin deficiency
Usually encountered in the first 3 months of life
Results from a variety of etiologiesc
Cheng L, Bostwick DG, eds. Essentials of Anatomic Pathology. 2nd Ed. Totowa, NJ: Humana Press; 2006: 1409.