
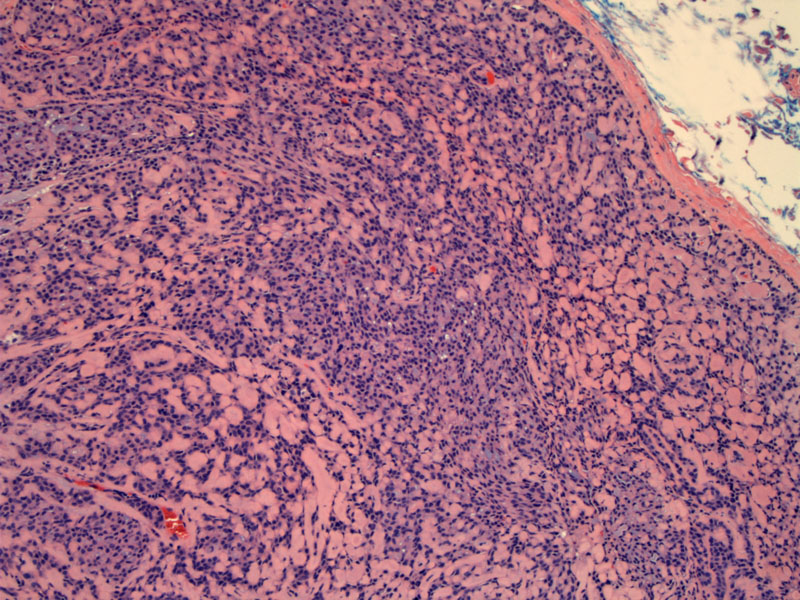
Basal cell adenomas of the major salivary glands are well encapsulated as seen here. In the minor salivary glands, the tumor may be unecapsulated (Brandwein).
){kind=link}
At higher power, excessive balls of eosinophilic basement membrane can be appreciated.
){kind=link}
The nuclei of the basaloid cells are pushed to the periphery from the elaboration of abundant hyaline material
){kind=link}
Tumor capsule interfaces with normal parotid (bottom image).
){kind=link}
There is variable 1-2+ c-kit staining in this BCA. C-kit expression is seen in adenoid cystic carcinoma, polymorphous low grade adenocarcinoma and monomorphic adenomas and thus, is not useful in distinguishing between these three entities (Edwards).
){kind=link}
Focal variable 2+ SMA highlights the myoepithelial (peripheral or abluminal basaloid).
){kind=link}
Keratin AE1/3 highlights the epithelial (luminal) component.
){kind=link}
Aspiration of this lesion shows aggregates of basaloid cells.
){kind=link}
PAS highlights the abundant hyaline basement membrane material.
){kind=link}
Basal cell adenoma is a subtype of monomorphic adenoma that is uncommonly seen and represents only about 2% of salivary gland tumors (Brandwein). About 70% arise in the parotid glands and 10-20% in the upper lip.
Like pleomorphic adenomas, these tumors typically present as discrete, mobile, non-painful masses. There are four main histologic subtypes: solid, trabecular, tubular and membranous.
The membranous subtype of basal cell adenoma, also known as a dermal analogue tumor, is a distinct variant morphologically similar to cylindromas (cutaneous adnexal tumors). In contrast to the other histologic subtypes which are solitary, membranous BCA grow in a multifocal and multinodular fashion.
This membranous basal cell adenomas may be seen in the context of the autosomal dominant salivary gland-skin adnexal tumor syndrome, a.k.a. Brooke-Spriegler syndrome. Patients develop hundreds of dermal cylindromas ("turban tumor"), trichoepitheliomas, eccrine spiradenomas as well as similar tumors in the salivary gland. The culprit germline mutation involves CYLD (cylindromatosis gene), a tumor suppresor gene located at chromosome 16q12-q13 (Yu, Fletcher).
Membranous adenomas usually arise in the parotid. Basal cell carcinomas generally arise in the 7th decade with a 2:1 female predilection. However, membranous adenomas have an equal gender distribution.
Paroditectomy with preservation of the facial nerve is the treatment of choice for this lesion. There is has been reportedly a higher rate of recurrence associated with the membranous subtype of this tumor due to its multifocal nature (Brandwein, Fletcher).
• Salivary Gland : Basal Cell Adenoma, Trabecular Type?
• Salivary Gland : Basal Cell Adenoma, Solid Type
Brandwein-Gensler M. Head and Neck: Illustrated Surgical Pathology Series. New York, NY: Cambridge University Press; 2010: 286-293.
Edwards PC, Bhuiya T, Kelsch RD. C-kit expression in the salivary gland neoplasms adenoid cystic carcinoma, polymorphous low-grade adenocarcinoma, and monomorphic adenoma.
Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003 May;95(5):586-93.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 255-7.
Yu GY, Ubmüller J, Donath K. Membranous basal cell adenoma of the salivary gland: a clinicopathologic study of 12 cases. Acta Otolaryngol. 1998 Jul;118(4):588-93.