
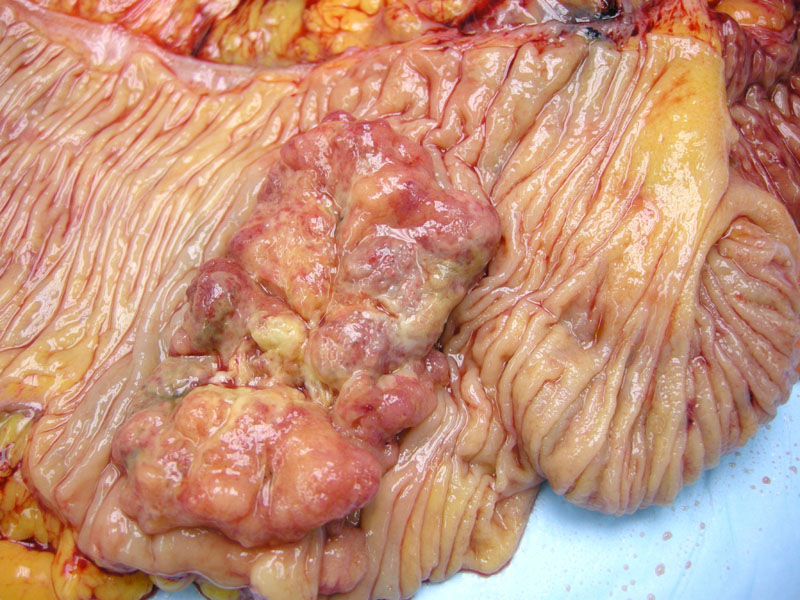
Grossly, right-sided colon cancers tend to be exophytic, polypoid (mushroom-like) masses. Due to the more accommodating cecum and ascending colon, right-sided tumors rarely cause obstruction.
){kind=link}
In contrast, the distal left-sided tumor demonstrates a constricting circumferential lesion -- obstructive symptoms likely to follow.
){kind=link}
Endoscopic imaging reveals an exophyic fungating mass with surface exudate nearly filling the lumen.
){kind=link}
Normal glands are located in the bottom image contrasted with malignant glands at the top.
){kind=link}
Where the neoplasm arose from -- note the benign gland at the left upper corner. The malignant cells have prominent nucleoli and loss of polarity.
){kind=link}
This was a stage T2 neoplasm that dissected into muscularis propria.
', 'micro', '')){kind=link}
In this separate case, a poorly-differentiated area can be appreciated. There is barely any recognizable gland formation.
){kind=link}
This particular tumor has invaded beyond the muscularis propria and into fat -- but has not yet breached the serosal surface (stage T3).
', 'micro', '')){kind=link}
Invasive glands often elicit extensive desmoplasia.
){kind=link}
Lymphovascular invasion is demonstrated here.
){kind=link}
Here is a different tumor with copious mucin production and well formed glands. Note that mucinous glands must comprise over 50% of the tumor to be called a mucinous adenocarcinoma.
){kind=link}
Dirty necrosis consists of eosinophilic necrotic debris -- it is commonly found within neoplastic glands.
){kind=link}
Another example of a poorly-differentiated (higher grade) colorectal adenocarcinoma consisting of solid areas of malignant cells.
){kind=link}
The tumor cells are draped around the periphery of a dilated gland, the so called garland pattern.
){kind=link}
Nuclear CDX2 positivity is demonstrated in this liver biopsy for metastatic colon cancer.
){kind=link}
Keratin 20 positivity is typical of colorectal adenocarcinoma.
){kind=link}
The tumor is generally not reactive for CK 7.
){kind=link}
Gene sequencing searches for mutations of codon 12 and 13 of the KRAS gene. The unmutated (wildtype) sequence ought to be GGT (codon 12) and GGC (13), as demonstrated here. Note the grey box at the top of the image highlighting the codons of interest.
){kind=link}
This sequence demonstrates a mutation at codon 12. Note the red box alerting the presence of dual signals at the top of the image. Below this red box, you will see two signals -- one in black and one in green. This confers a GGT to GAT mutation. This patient is not a candidate for anti-EGFR therapy.
){kind=link}
Colorectal cancer is the third most common cause of cancer deaths among men and women in the United States. Peak incidence for colorectal carcinoma occurs between age 60-79. A 'Western' lifestyle of inactivity plus a refined, low-fiber, high-cholesterol diet has been implicated as a significant risk factor. Most colon cancers occur sporadically, but a significant minority (estimates range from 3-10%) occur in patients with familial syndromes (FAP or HNPCC) or in the setting of inflammatory bowel disease such as ulcerative colitis. Thus, if a patient presents with colorectal carcinoma prior to age 50, one must suspect an inherited disposition or inflammatory bowel disease.1,2
The majority of colorectal cancers (55%) occur in the rectosigmoid, followed by the cecum/ascending colon (22%), transverse colon (11%), descending colon (6%) and other sites (6%). Note that depending on age, sex, ethnicity and genetic mutations, right-sided or left-sided lesions predominate. To be overly simplistic, right-sided lesions are more common in low-risk countries, women, African-Americans and patients with HNPCC. Left-sided lesions are more common in high-risk.
Microscopically, colorectal carcinomas are categorized into well-differentiated, moderately differentiated and poorly differentiated. In well-differentiated tumors, tubule formation is present in greater than 75% of the tumor. The epithelium is similar to an adenomatous polyp, with thin cigar-shaped nuclei that retain polarity. Moderately differentiated carcinomas still exhibit tubule formation, but the glands are less regular and display increasing architectural complexity (cribriforming and budding blands). Poorly differentiated tumors have less than 25% gland formation with malignant cells in sheets -- the nuclei tend to be round, pleomorphic with prominent nucleoli and complete loss of polarity. Areas of dirty necrosis (eosinophilic necrotic material) with malignant glands are often seen.2,3
Right-sided colon cancers that arise via the microsatelllite instability pathway will be discussed as a separate case (see below) -- note that these tumors may exhibit a particular histology.
IHC studies demonstrate positivity for LMW keratins (AE1/AE3, CAM5.2), EMA, CEA and CK20. Tumors demonstrate variable positivity for CK7 and are negative for vimentin.2
Colon cancer can be notoriously insidious, remaining asymptomatic for years. As mentioned above, due to the differences in right-sided and left-sided lesions, right-sided lesions rarely cause obstruction and may be clinically silent. Left-sided lesions tend to present with diarrhea, decrease in stool caliber, tenesmus and incontinence.
As drilled into all medical students, "an older male with iron-deficiency anemia has colon cancer until proven otherwise!". In females, the situation is less clear because menstruation and abnormal uterine bleeding can also cause anemia. Fatigue, malaise and weight loss indicate advanced disease. 50% of patients present with bleeding -- frank bleeding is more common in left-sided lesions and dark, maroon-colored stools would indicate a right-sided lesion.
Surgical resection is effective for stage 1 or 2 cancers. Adjuvant therapy is employed for advanced stage cancers. These adjuvant chemotherapies largely consisted of 5-fluorouracil, irinotecan and oxaliplatin.
A note about KRAS: The newly developed anti-EGFR antibodies (cetuximab or panitumumab) are chemotherapies that have shown promise in the treatment of refractory, metastatic colorectal carcinoma and prolonging survival. The EGFR signaling pathway plays an important role in carcinogenesis, as this pathway is overactive in 80% of colorectal carcinomas. Antibodies to EGFR block this pathway and its downstream effects (celluar proliferation, angiogenesis, cell migration).4
Studies have shown that 30-40% of patients with colorectal cancers have a KRAS mutation that render them resistant to anti-EGFR therapy. The KRAS mutation, located on codon 12 or 13 of the KRAS gene, causes a constitutive activation of the protein, thus, blocking the EGFR pathway via cetuximab upstream using anti-EGFR therapy is ineffective. Therefore, prior to initiating anti-EGFR therapy, most clinicians request the KRAS status of the patient. Mutations can be identified using gene sequencing.4
Stage is the most important prognostic factor. The 5 year survival rate for early stage (localized) colorectal carcinoma is approximately 90%, however, up to 30% of cases present at advanced stages, when the disease is not surgically resectable. The 5 year survival rate drops to 68% when regional spread occurs and down to 10% with distant metastases.4 Thus, routine surveillance via colonscopy is important to identify and remove adenomatous polyps.
Colorectal cancers spread by direct extension into adjacent structures and via metastasis through lymphovascular channels. Favored sites of metastasis include lymph nodes, liver, lungs and bones (in that order).
• Colon : Adenocarcinoma, Mucinous Signet Ring Type
• Colon : Adenocarcinoma, Mismatch Repair Related
• Vulva : Adenocarcinoma from Colon
• Colon : Mucinous Adenocarcinoma
• Colon : Tubulovillous Adenoma
• Colon : Adenocarcinoma, Mucinous Signet Ring Type
1 Kumar V, Abbas AK, Fausto N. Robbins and Cotran Pathologic Basis of Disease. 7th Ed. Philadelphia, PA: Elsevier; 2005: 864-6.
2 Iacobuzio-Donahue CA, Montgomery EA. Gastrointestinal and Liver Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier; 2005: 382-5.
3 Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 397-403.
4 Monzon FA, Ogino S, Hammond EH et al. The Role of KRAS Mutation Testing in the Management of Patients With Metastatic Colorectal Cancer. Arch Pathol Lab Med. 2009;133:1600-6.
***Gene sequencing images courtesy of Joseph Pierce, Molecular Diagnostics at Tricore Reference Laboratories, Albuquerque NM.
***Gross images courtesy of Myra Zucker, Dept of Pathology at University of New Mexico, Albuquerque NM.