System: Breast: Lobular: Malignant: Infiltrating Lobular Carcinoma


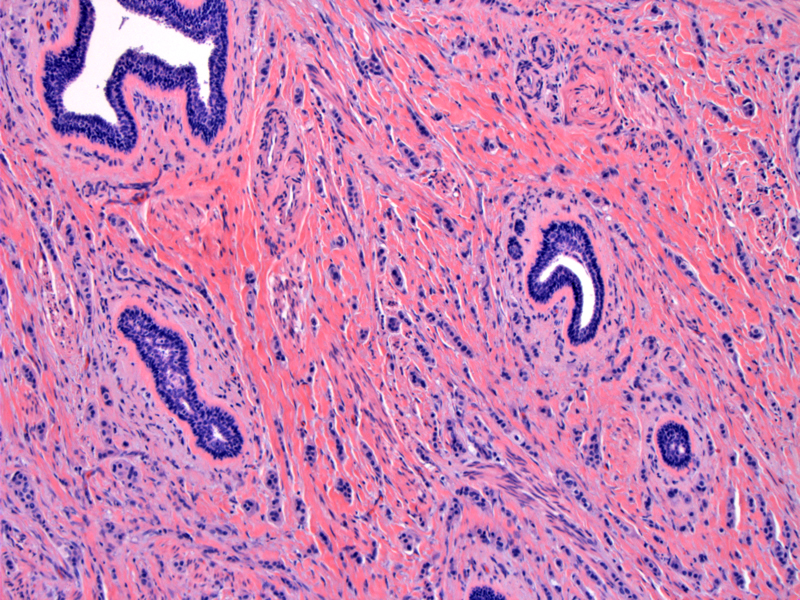
Between normal appearing ductal structures are linearly arranged streams of round cells.
The hallmark of infiltrative lobular carcinoma is the single-filing of tumor cells. Desmoplastic response may be minimal or absent.
A higher power of single-filing cells. The nuclei are generally small, round or oval, sometimes with eccentrically placed nuclei, giving a signet ring look. In this image, there is little pleomorphism and no mitotic figures, favoring the diagnosis of the classic type of lobular carinoma.
For comparison, this example which shows infiltrating ductal carcinoma with areas of lobular growth pattern. Note that the these files are more than one cell in width, streaming through a desmoplastic stroma.
The cell block clearly demonstrates the discohesiveness of the lesional cells.
ER stain on cell block demonstrates ER positivity. Note that most lobular carcinomas are ER and PR positive with no Her2/neu overexpression. These features are flipped in pleomorphic, high-grade lesions.
Low power very cellular Image
some patternless, some lining up Image
a few cells with cytoplasmic mucin vacuole Image
Invasive lobular carcinomas constitute ~10-15% of invasive breast cancers and is the second most common form of invasive breast cancer. Bilaterality and multicentricity are purported features of lobular carcinomas, however, these issues are still being disputed. The higher likelihood of contralateral mastectomy in women with lobular carcinomas may have created a biased picture. The incidence of lobular carcinomas appear to be rising, possibly due to hormonal replacement therapy in post-menopausal women.1,2
There are several histologic variants of lobular carcinomas which have important prognostic implications.
Well-differentiated and moderately differentiated lobular carcinomas express ER and PR receptors, without overexpression of HER2/neu. However, poorly-differentiated lobular carcinomas lack ER and PR receptors and may overexpress HER2/neu. Lobular carcinomas and LCIS demonstrate loss in a region of chromosome 6 responsible for cell-adhesion, which includes the genes for e-cadherin and B-catenin. Inactivation (by mutation or methylation) of e-cadherin on the opposite allele results in a lack of e-cadherin expression.1,3
Presents similarly to NST as a palpable mass or a density on mammogram, however, a minority of cases may present as a vague, ill-defined thickening of the breast with subtle changes on mammogram due to an infiltrative tumor without a desmoplastic response.2 Also, there is less of an association with microcalcifications than NST.
The histologic subtype is a prognostic factor. The tubulo-lobular variant has the most favorable outcome of the group, with a 17% risk of local recurrence and 13% risk of distant metastasis. In comparison, the solid variant has a 82% risk of local recurrence and 54% risk of distant metatstasis. The 12 year survival of tubulo-lobular variant is 100% versus 47% for the solid subtype.2 The pleomorphic variant carries a worse prognosis, as it is a variant with high-grade features by definition.
Lobular carcinomas have a unique pattern of metastasis, favoring the the GI tract, ovaries, leptomeninges, uterus and CSF. They do not favor the lungs and pleura (like NST).
• Lobular : Lobular Carcinoma in Situ, Pleomorphic Variant
1 Kumar V, Abbas AK, Fausto N. Robbins and Cotran Pathologic Basis of Disease. 7th Ed. Philadelphia, PA: Elsevier; 2005:1144-5.
2 O'Mallye FP, Pinder SE. Breast Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elvesier; 2006:203-6.
3 Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 931-2.
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}