
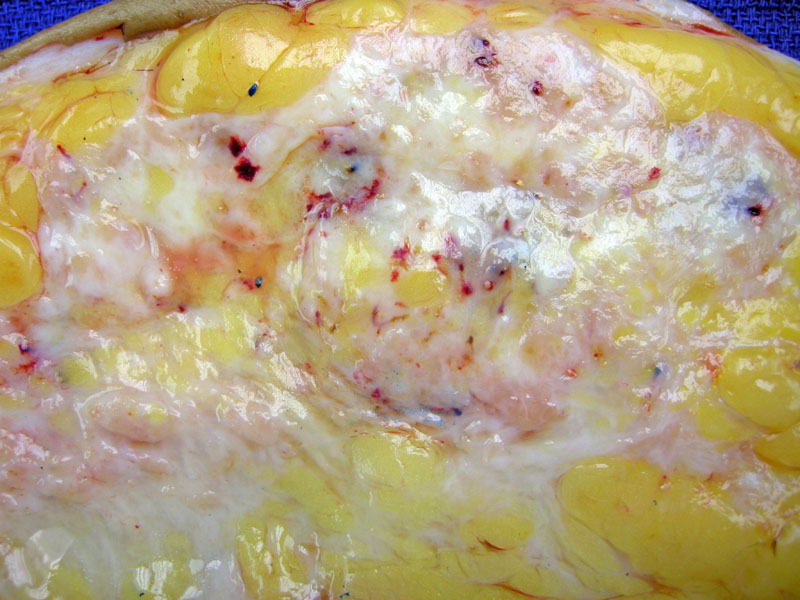
Gross image of a 20 cm mass that was a moderately differentiated ductal carcinoma.
The borders of a ductal carcinoma are ill-defined and infiltrative.
At high power, the tumor shows nodular growth and solid foci which are clearly firm and distinct from fibrocystic change.
Case 1: Well-differentiated ductal carcinoma: angulated tubules, limited solid areas, marked desmoplasia are present
No marked pleomorphism or mitotic activity along with extensive tubule formation corresponds to a diagnosis of grade I or well-differentiated ductal carcinoma.
The (well-differentiated) tumor cells form small clusters in cell block.
Case 2: An example of moderately differentiated invasive ductal carcinoma. The nuclei are not overly atypical, but tubule formation is scant.
Case 3: An example of poorly differentiated invasive ductal carcinoma. The nuclei are more pleomorphic, tubule formation is lacking, and mitotic figures are not hard to find.
In poorly differentiated IDC, there is marked nuclear pleomorphism. Nuclei are markedly enlarged and more variable, with vesicular dark chromatin.
As well as a high mitotic count.
Dermal lymphatic spread of tumor is considered by some to be a poor prognostic factor.
Several tumor filled lymphatic channels are highlighted by D2-40 .
Lymph node with subcapsular micrometastasis (right of center).
FNA of lymph node with metastatic ductal carcinoma -- lymphoid cells are present in background of large irregular cohesive groups of much larger malignant cell).
Another example of an aspirated lymph node with ductal carcinoma.
Metastatic ductal carcinoma in pleural fluid with mesothelial cells in the background.
Cohesive cluster of ductal adenocarcinoma in a cell block generated from the above pleural fluid.
Strong HER-2/neu expression predicts response to trastuzumab (Herceptin). HER2-positive cases accouns for 25 to 30% of all breast cancers. Clinically, HER2-positive tumors are associated with a more aggressive subtype, and poor outcomes.
Infiltrating skin metastasis at scar site - note the desmoplasia alongside the keloidal collagen.
Cancerization of lobules by ductal carcinoma can be appreciated here.
Invasive carcinomas of the breast are largely divided into those with special histology (e.g. lobular, medullary, mucinous, tubular) and those without a specific histology. The latter is known as invasive ductal carcinoma -- some authorities prefer the term "infiltrating ductal carcinoma of no special type" or "infiltrating ductal carcinoma, not otherwise specified".
To be classified as an invasive carcinoma with special histology (e.g. tubular carcinoma), the defining histologic features should be present in at least 90% of the tumor. By far, the largest group of breast carcinomas are IDC, comprising 50 to 75% of cases. Lobular (5-15%), medullary (3-9%), mucinous (1-2%), tubular (1-3%), mixed and other rare subtypes account for the rest of invasive breast cancers (Mills).
Grossly, IDC has a stellate, irregular, infiltrative outline. There is a very firm and hard feel to the tumor. Histologically, infiltrative glands are arranged in sheets, cords and trabeculae. The myoepithelial layer is largely absent (Fletcher, Mills).
Histologic grading -- "Nottingham grade" -- gives a numerical score (1-3) in three dimensions: mitotic activity, tubule formation and nuclear pleomorphism. A score of 3-5 is well differentiated, 6-7 is moderately differentiated and 8-9 is poorly-differentiated.
Some other features include squamous metaplasia, areas of necrosis, neuroendocrine differentiation (~10% of cases), which carry no prognostic significance.
Treatment options are generally based on TNM staging. Lymphovascular spread, histologic grade, hormone receptor status, HER2/neu overexpression, comorbidities, and patient menopausal status and age are also relevant.
For those who qualify for breast conserving local excision, radiation is often recommended to treat subclinical disease. A review of 10 randomized controlled trials comparing breast-conserving surgery with and without radiation showed that radiation in addition to surgery significantly reduces the 5-year local recurrence rate (Clarke).
Chemotherapy is the standard of care for node-positive cancer or for tumors larger than 1 cm. Hormone receptor–negative disease derives a greater benefit from chemotherapy than hormone receptor–positive disease (Goldhirsch).
Prognostic factors (assesses outcome at time of diagnosis) include lymph node metastasis, tumor size, histologic type, histologic grade, lymphatic vessel spread as well as markers of proliferation (e.g. Ki-67), oncoproteins (e.g. HER2/neu), and tumor suppresor genes (e.g. p53).
Predictive factors (assesses likelihood of response to therapy) include ER, PR status as well as HER2/neu expression (Mills).
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 929-930.
Mills SE, ed. Sternberg's Diagnostic Surgical Pathology. 5th ed. Philadelphia, PA: Lippincoott Williams & Wilkins; 2009: 318-321.
Clarke M, Collins R, Darby S, et al.; Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;366(9503):2087–2106.
Goldhirsch A, Wood WC, Gelber RD, Coates AS, Thürlimann B, Senn HJ. 10th St. Gallen conference. Progress and promise: highlights of the international expert consensus on the primary therapy of early breast cancer 2007 [published correction appears in Ann Oncol. 2007;18(11):1917]. Ann Oncol. 2007;18(7):1133–1144.

){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}