System: Gastrointestinal: Small Intestines: Infectious: Strongyloides

System: Gastrointestinal: Small Intestines: Infectious: Strongyloides

Case 1: Strongyloides affects the glandular epithelial cells, and a host inflammatory response is lacking. Some cases do show a neutrophilic infiltrate
Strongyloides is seen better at high power in the duodenal epithelium.
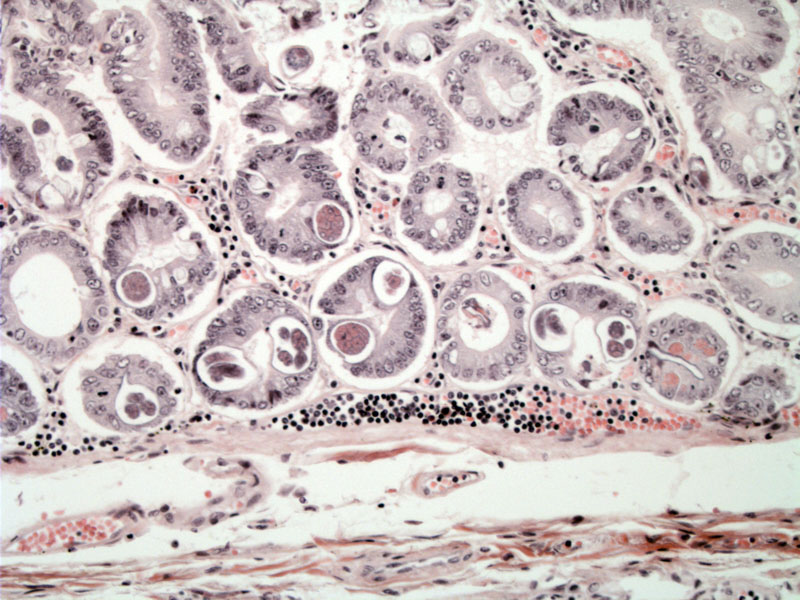
Case 2: Both the adult worm and larvae may be found in crypts. Both forms can be appreciated here.
There may be a vigorous eosinophilic and neutrophilic infiltrate, as seen here in the submitted duodenal biopsy.
Strongyloides stercoralis is a nematode found anywhere in the world. In the US, it is endemic in SE urban areas and in mental institutions. The organism penetrates the skin, enters the venous system, goes to the lungs and migrates up respiratory tree down into esophagus to set up in the small intestines. The females lays eggs in small intestines, where the parasite can resides for up to 30 years due to the cycle of autoinfection.
Autoinfective larvae penetrate the wall of the ileum or colon or the skin of the perianal region, enter the circulation again, travel to the lungs, and back down to the small intestine, thus repeating the cycle.
Endoscopically, one may find hypertrophic mucosal folds and ulcers. Microscopically, both adult worms and larvae may be found in the crypts. The adult worm has sharply pointed tails that may be curved. Other histologic features include villous blunting, ulcers, edema and a dense eosinophilic and neutrophilic infiltrate.
Strongyloides infection may be asymptomatic for years, due to a low parasite load. If cellular immunity is depressed, autoinfection can occur at a higher rate, resulting in hyperinfection syndrome. Patients with immunodeficiency or taking steroids are therefore most likely affected.
Infected individuals may manifest diarrhea, abdominal pain and tenderness, nausea, vomiting, or GI bleeding; one may also see rash, eosinophilia, urticaria, and pulmonary symptoms, while some patients may even be asymptomatic. The organisms can also involve stomach and large intestines.
The disease may be managed with anthelminthic drugs, including ivermectin.
If untreated, the hyperinfection syndrome caused by Strongyloides stercoralis has a high mortality rate (15% to 87%.)
){kind=link}
){kind=link}
){kind=link}
){kind=link}