
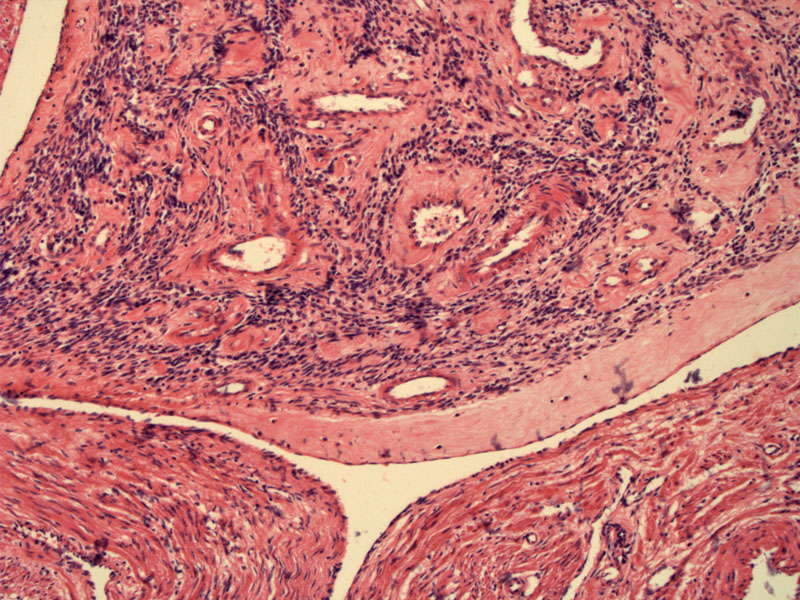
The leiomyoma has filled the vascular space. The outline of the vascular space is seen in the periphery of the image, and the neoplasm fills most of the center of the image.
){kind=link}
A closer inspection reveals complete absence of mitoses and atypia in the leiomyoma. Note the thick walled vessels.
){kind=link}
Areas of the tumor are edematous, hypocellular and collagenized.
){kind=link}
Not only do leiomyomas have a vast array of histologic subtypes, but these neoplasms can also have very odd growth patterns. Some names given to these entities include:
Intravenous leiomyomatosis -- leiomyomatous tissue extends beyond the confines of the leiomyoma and one may see worm-like plugs of tumor in parametrial vessels.
Leiomyomatosis peritonealis disseminata-- multiple nodules of leiomyomatous tissue on peritoneal surfaces usually seen in black and pregnant women
Diffuse leiomyomatosis -- numerous small myomas that merge together and diffusely involve and expand the myometrium.
Benign metastasizing leiomyoma -- metastatic leiomyomatous deposits are found in the lung or lymph nodes; patients usually have concurrent leiomyomas or a history of hysterectomy or myomectomy for leiomyomas (Silverberg).
Note that in all these entities, the displaced leiomyomatous tissue is benign with bland histology similar to the uterine counterpart. Features of leiomyosarcoma (mitotic activity, necrosis, etc) must be excluded (Sternberg).
The main differential diagnosis for intravascular leiomyomas is endometrial stromal sarcoma (older term: endolymphatic myosis), which has a propensity to involve lymphovascular channels. Intravascular leiomymomas should exhibit larger vessels, whereas the vascular background in endometrial stromal sarcomas has a 'arborizing' pattern of delicate sometimes hyalinized vessels. Furthermore, intravascular leiomymomas often have a clefted like contour, which is lacking in endometrial stromal sarcomas. In difficult cases, IHC may be helpful as endometrial stromal tumors do not stain with muscle markers such as h-caldesmon (Fletcher).
Typically present with abnormal uterine bleeding, pelvic pain and an enlarged uterus. Upon gross inspection, worm-like tumor plugs within vessels may be seen. In most instances, a concurrent leiomymoma is found in the uterus, however, in some instances, the tumor exists entirely within vascular spaces. Rarely, the neoplasm may extend into the inferior vena cava and enter the right atrium!
Most cases of intravascular leiomyomatos are benign and indolent. In cases of leiomyoma with vascular invasion, excision of the tumor or a hysterectomy is curative. In cases of extrauterine extension, there is a risk of recurrence. Treatment has not been standardized because of this entity is uncommon. Lam and colleagues (2004) found 200 cases of intravenous leiomyomatosis in the medical literature between 1980 to 2003. Of these, 68 were of intracardiac leiomyomatosis (ICL). Vascular surgery was employed in the majority of the ICL cases. Complete excision is the treatment of choice to prevent recurrence. Removal of the ovaries is also necessary as these tumors are hormonally driven (Lam).
In terms of benign metastasizing leiomyoma, treatment depends largely on tumor volume and sites involved. Again, it is very rare, so no standardized treatment has been developed. Reported treatments have included observation, resection, hysterectomy and bilateral oophorectomy, progesterone, and medical castration using luteinizing hormone-releasing hormone analogue.
• Myometrium : Leiomyoma, Mitotically Active
• Endometrium : Intravascular Endometrium
• Myometrium : Endometrial Stromal Sarcoma, Low-Grade
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 692-3.
Lam PM, Lo KW, Yu MY et al. Intravenous leiomyomatosis: two cases with different routes of tumor extension. J Vasc Surg 2004 Feb;39(2):465-9.
Silverberg SG. Silverberg's Principles and Practice of Surgical Pathology and Cytopathology. Philadelphia, PA: Elsevier; 2006: 1973.
Sternberg SS, ed. Diagnostic Surgical Pathology.4th Ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2004: 2519-2520.