
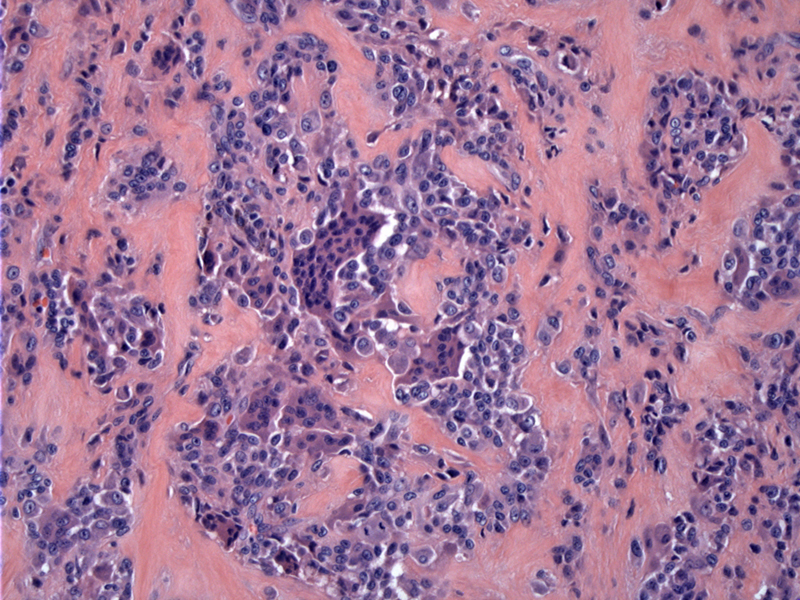
The tumor is composed of an admixture of multinucleated giant cells and rounded synovial-like stromal cells.
){kind=link}
The stroma can be heavily hyalinzed (or collagenous), outlining each individual or groups of cells.
){kind=link}
Giant cells may also take the form of so-called Touton giant cells, with nuclei forming a wreath around the pink cytoplasm.
){kind=link}
Foamy macrophages arise in clusters, as seen here by numerous medium sized cells with clear frothy cytoplasm and indistinct nuclei. When abundant, the possibility of a tendinous xanthoma may be considered.
){kind=link}
The tumor is fairly well-localized in this example, with a distinct pseudocapsule (right)
){kind=link}
Giant cell tumor of tendon sheath arises from the synovium and occurs in two forms: a localized form and diffuse form. The many names ascribed to this tumor has been a source of confusion. The localized form is also known as nodular tenosynovitis or tenosynovial giant cell tumor, localized type and the diffuse form is often referred to as pigmented villonodular synovitis (PVNS) or tenosynovial giant cell tumor, diffuse type (Weiss, Mills). However, all names (especially old historical names) provide information regarding the entity. For example, from the aforementioned names, we can surmise that giant cells, tendon, synovium and pigmentation will all probably be important features of the lesion.
The localized (or nodular) form is a small circumscribed mass usually located in the digits, with fingers outnumbering toes by 10:1 (Fletcher). The diffuse type most commonly affects the knee. Grossly, the localized type is firm, well-circumscribed nodule. The diffuse type (PVNS) is seen as a diffuse thickening of the synovium - multiple nodules as well as papillary and villous excrescences are present. The cut surfaces may be yellow or brown, depending on the amount of lipid or hemosiderin.
Microscopically, there are numerous multinucleated giant cells admixed with inflammatory cells (especially histiocytes and lymphocytes) and rounded mononuclear stromal cells. The stroma can be heavily collagenous or hyalinized, especially the localized form. Hemosiderin or lipid-laden macrophages are commonly present.
The macrophages and multinuclated giant cells will stain with CD68, and the mononuclear cells may be reactive for Ham56, PGM1 and MAC387 (Folpe). 60-70% of the giant cell tumor of tendon sheath (both localized and diffuse) contain a unique translocation. The fusion of colon-stiumlating factor-1 gene (CSF1) on 1p13 to the collagen VI (COL6A3) gene on 2q35, produces COL6A3-CSF1(Weiss, Folpe).
This fusion gene produces a large amount of CSF1, a potent chemoattractant for macrophages. Thus, numerous histocytes, multinucleated giant cells, lymphocytes and other inflammatory cells are recruited by the neoplastic tissue.
The localized form is more common in women (F:M ratio of 2:1) with peak incidence in the second through fourth decades. There is no gender predilection in the diffuse form.
The vast majority of the localized tumors occur in the fingers. Other sites include the toes and rarely, in larger joints such as ankle/foot and knee. In contrast, the large joints (knee, ankle, wrist elbow) are the favored location of the diffuse type. The history is often that of a slow-growing mass, often remaining the same size for many years.
Local excision with a small cuff of normal tissue is optimal.
These lesions are now considered to be neoplastic, however, the course is generally benign and excision is curative in most cases. There is a recurrence rate of 10-20%, which is treated with re-excision. Rarely, the mass may lead of cortical erosion of bone.
→Giant cell tumor of tendon sheath comes in two flavors: localized and diffused.
→The localized form is nodular and circumscribed, most often arising in the fingers.
→The diffuse form (a.k.a pigmented villonodular synovitis) is diffusely nodular with villous and finger-like projects, most often arising in the knee joint.
→Both the diffuse and localized forms are associated a translocation that produces the COL6A3-CSF1 fusion gene.
• Joints : Pigmented Villonodular Synovitis
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 1558.
Folpe AL, Inwards CY. Bone and Soft Tissue Pathology: Foundations in Diagnostic Pathology Philadelphia, PA: Elsevier; 2010: 255-261.
Mills SE, ed. Sternberg's Diagnostic Surgical Pathology. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009: 173.
Weiss SW, Goldblum JR. Enzinger. Enzinger and Weiss' Soft Tissue Tumors. 5th Ed. Philadelphia, PA: Elsevier; 2008: 770-777.