
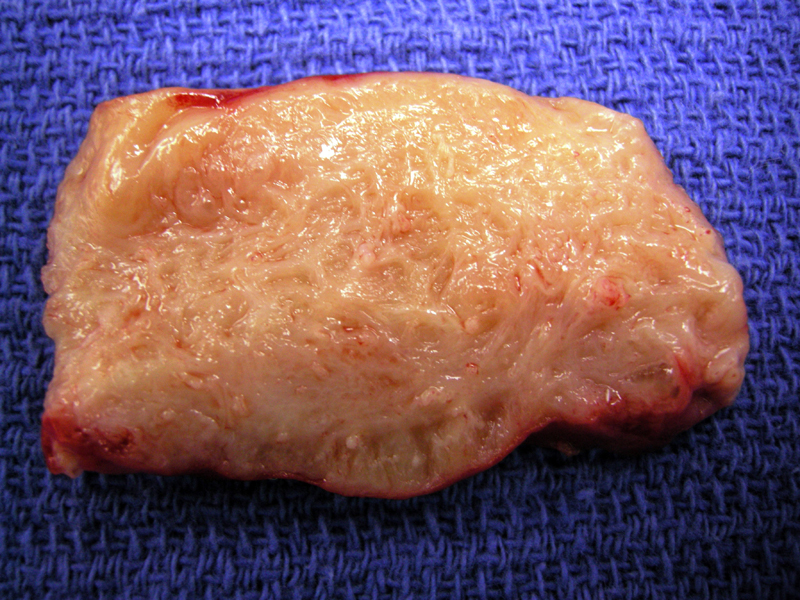
Cross section of uterine wall shows a trabeculated surface with glistening appearance consistent with adenomyosis.
){kind=link}
Endometrial tissue consisting of endometrial glands and stroma are embedded within the myometrium. The glands tend to have a basalis appearance (tubular and weakly proliferative).
){kind=link}
Another example demonstrates endometrial glands and a rim of endometrial stroma surrounding by fascicles of smooth muscle.
){kind=link}
Adenomyosis immediately underlies normal surface endometrium. Much of the myometrial wall was involved.
){kind=link}
Adenomyosis is defined as endometrial glands and stroma within the myometrium. Endometrial tissue (glands and stroma) located within the myometrium is called adenomyosis. If located in the uterine serosa and outside the uterus, it is termed endometriosis.
In many cases, the microscopic diagnosis of adenomyosis is simple. Endometrial glands and endometrial stroma are found deep within the myometrium. However, more superficial adenomyosis may be difficult to detect for two reasons: (1) tangential cuts of uterine tissue may mimic adenomyosis and (2) the junction between endometrium and myometrium is jagged and irregular, thus, it may be difficult to determine if the endometrial tissue is actually within the myometrium. Thus, some authors propose that a rim of hypertrophied smooth muscle be must surround the endometrial tissue to secure the diagnosis. This requirement is not necessary if adenomyosis is deep within the myometrium.
Occurs in reproductive age women. The classic patient is a parous reproductive age woman with a late onset of menorrhagia and dysmenorrhea. On exam the classic description is of a "boggy" enlarged tender uterus.
Grossly, diffuse adenomyosis leads to lead to a 'globoid' enlargement of the uterus. The cut surface is trabecular. Unlike leiomyomas, adenomyosis is usually a diffuse non-circumscribed process and cannot be easily shelled out.
Treatments can be medical or surgical. Medical treatments involve hormonal suppression of endometrial growth. Definitive therapy consists of a hysterectomy.
Benign.
1 Mills SE, ed. Sternberg's Diagnostic Surgical Pathology.4th Ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2004: 2503-4.
2 Kurman RJ, Norris HJ, Wilkinson E. Tumors of the Cervix, Vagina and Vulva: Atlas of Tumor Pathology. Third Series Fascicle 4. Washington DC; AFIP: 1990: Section 9.3.