
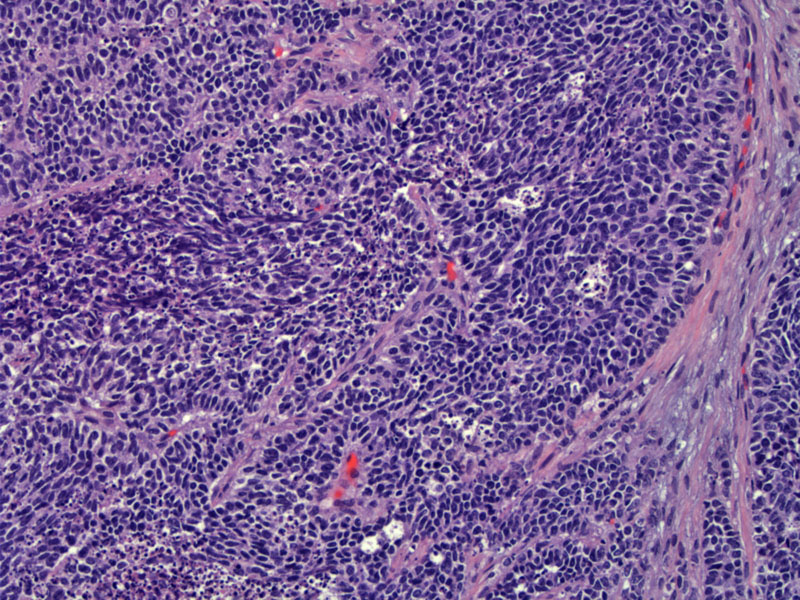
Small cell neuroendocrine carcinoma (SCNC) grows in solid, insular, nested or trabecular patterns. This image demonstrates small round blue cells growing in diffuse sheets with areas of poorly formed trabeculae.
){kind=link}
The malignant cells exhibit high N/C ratios and a finely stippled chromatin pattern. The nucleoli are inconspicuous. Nuclear molding and numerous apoptotic bodies are seen. Necrosis is also a common feature. The confluent area of apoptotic bodies seen in the right image can probably be called necrosis.
){kind=link}
A normal residual endocervical gland (lower right) is seen adjacent to an infiltrate of tumor cells. Note again the prominent nuclear molding and apopotic bodies.
){kind=link}
Neuroendocrine tumors consist of carcinoid, atypical carcinoid, large cell and small cell neuroendocrine carcinomas, all of which can affect the cervix. Small cell carcinoma is the most common neuroendocrine tumor of the cervix, accounting for 5% of all cervical carcinomas.
Small cell neuroendocrine carcinomas (SCNC) are histologically identical to those that occur in the lung, however, up to 80% of cervical SCNC is associated with high-risk HPV subtype 18 (Ishida).
SCNC must be distinguished from poorly differentiated nonkeratinizing squamous cell carcinoma and basaloid squamous cell carcinoma. Although the latter two entities are composed of small cells with high N/C ratios, they do not exhibit features characteristic of SCNC such as nuclear molding and crush artifact. Neuroendocrine markers may also be helpful, as SCNC will demonstrate positivity with chromogranin, synaptophysin and neuron-specific enolase. Lymphoma will also be on the differential, and this entity will grow in diffuse sheets and exhibit markers of B-cell lineage.
Average age of presentation is between 36-42 and may present with vaginal bleeding or paraneoplastic syndrome (ie. Cushing syndrome) as a result of peptide hormones produced by the tumor cells.
Treatment can be with surgical resection, radiation therapy, and chemotherapy. There is little data to suggest the best way to treat these tumors, though survival rates do suggest that surgical resection is a reasonable approach if possible.
Prognosis is grim. In one study, median survival for patients with early stage disease (IA1-IB2) was 31.2 months and 6.4 months for patients with advanced stage disease (IIB-IV) (Zivanovic).
• Endometrium : Small Cell Carcinoma
• Ovary : Small Cell Carcinoma, Hypercalcemic Type
Ishida GM, Kato N, Hayasaka T et al. Small cell neuroendocrine carcinomas of the uterine cervix: a histological, immunohistochemical, and molecular genetic study. Int J Gynecol Pathol. 2004 Oct;23(4):366-72.
Nucci MR, Oliva Esther. Gynecologic Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier: 2009: 188-190
Zivanovic O, et al. Small cell neuroendocrine carcinoma of the cervix: Analysis of outcome, recurrence pattern and the impact of platinum-based combination chemotherapy. Gynecol Oncol. 2009 Mar;112(3):590-3.