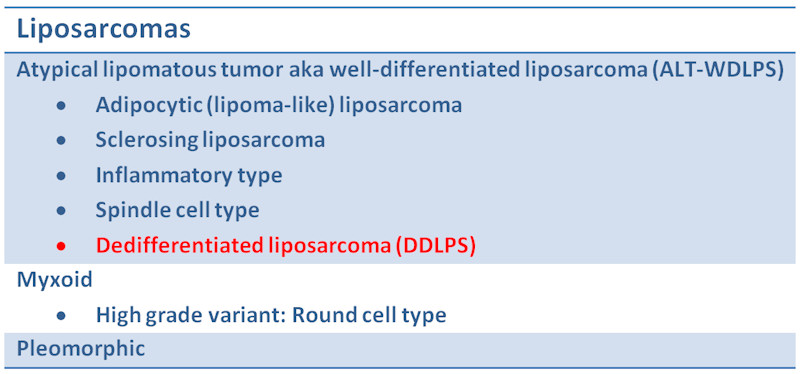
Categorization of liposarcomas
){kind=link}
The architectural pattern of the dedifferentiated component is generally a storiform pattern, resembling the so-called malignant fibrous histiocytoma. Foci of well-differentiated liposarcoma can usually be found with careful examination.
){kind=link}
CDK4 immunostain is good marker for DDLPS.
){kind=link}
MDM2 immunostain is another good marker for DDLPS.
){kind=link}
A recent study conducted by Binh and colleagues revealed that MDM2 and CDK4 consistently identified ALT-WDLPS as compared to benign lipomas. As you can see, 44 out of 44 ALT-WDLPS tumors stained positively with MDM2 and 40 of 44 staining positively with CDK4. With the exception of a few spindle cell and pleomorphic lipomas, none of the other benign lipomas stained MDM2 or CDK4.
){kind=link}
MDM2 and CDK4 was also extremely useful in distinguishing DDLPS from other simulator lesions. Note that MDM2 does stain a number of other entities such as MPNST and mxyofibrosarcoma, however CDK4 is more discriminate. Therefore, it would be best to order both stains.
){kind=link}
Gross specimen of a dedifferentiated liposarcoma is seen here, which shows a heterogeneous tumor with fleshy areas indicating sarcomatous transformation.
){kind=link}
Scattered pleomorphic cells are seen in the dedifferentiated region. The spindled proliferation does not indicate the origin of the tumor, so you must look for more conventional foci of liposarcoma.
){kind=link}
In other areas, the stroma is looser and more myxoid but the degree of atypia persists.
){kind=link}
S100 stains a few scattered cells, as would be expected from a lipomatous tumor. The stained cell in the lower part of the image could be a lipoblast.
){kind=link}
Dedifferentiated liposarcoma is considered to be a "variant" of well-differentiated liposarcoma. Histologically, the lesion consists of well-differentiated component with an abrupt transition to a dedifferentiated, high grade sarcomatous component. Well-differentiated liposarcomas do not metastasize, but well-differentiated liposarcomas with a dedifferentiated component has developed the capacity for metastasis.
Distinguishing lipoma-like liposarcomas from benign adipose tumors and distinguishing dedifferentiated liposarcomas (DDLPS) from poorly differentiated sarcomas has been problematic historically. For example, higher grade areas may look histologically similar to fibrosarcomas, malignant peripheral nerve sheath tumors (MPNST), so-called malignant fibrous histiocytomas and many other sarcomatous lesions.
The inital definition of dedifferentiated liposarcoma has been expanded over the years to now include dedifferentiation into exclusively low-grade areas or into a combination of low and high-grade areas. These lower grade variants can be diagnostically problematic, I must say, and require close scrutiny. Such tumors resemble fibromatosis or in some cases look similar to DFSP.
Fortunately, help comes in the form of two immunostains, MDM2 and CDK4. In simplified terms, all well-differentiated liposarcomas (ALT-WDLPS and DDLPS) exhibit an overamplication of genes on the long arm of chromosome 12, which contain MDM2 and CDK4. Staining for MDM2 and CDK2 will be positive in both well-differentiated liposarcomas as well as the dedifferentiated component.
Dedifferentiated liposarcoma is predominately located in the retroperitoneum and occasionally in the spermatic cord, head and neck region, or extremities. ~90% occur de novo and ~10% develop as a recurrence from an incompletely excised well-differentiated liposarcoma (Fletcher).
Metastasis occurs ~15-25% of dedifferentiated liposarcomas, regardless of the grade of the tumor. Recurrence is also not uncommon. Whether the dedifferentiated component contains bland fascicles of spindle cells or bizarre atypical cells does not affect the prognosis. 5 year survival rates for DDLPS is 60-70% (compared to 90% for well-differentiated liposarcoma)(Fletcher, Binh). These statistics are actually better than for those with other high grade sarcomas.
The most important prognostic factor in one study of 155 cases was tumor location, in that retroperitoneal tumors had worse survival than those in other sites (Hendricks). This study was not able to show that a low percentage of areas with dedifferentation had any impact on survival, in their study group.
• Lipomatous : Liposarcoma, Well-Differentiated Type (Atypical Lipomatous Tumor)
• Lipomatous : Liposarcoma, Pleomorphic Type
• Lipomatous : Liposarcoma, Myxoid Type
• Lipomatous : Liposarcoma, Well-Differentiated Type (Atypical Lipomatous Tumor)
• Uncertain Lineage : Synovial Sarcoma
• Myxoid : Myxofibrosarcoma, High Grade
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007:1536-7.
Binh MBN et al. MDM2 and CDK4 immunostainings are useful adjuncts in diagnosing well-differentiated and dedifferentiated liposarcoma subtypes. Am J Surg Pathol 2005;29:1340-7.
WH Henricks, et al. Dedifferentiated Liposarcoma: A Clinicopathological Analysis of 155 Cases with a Proposal for an Expanded Definition of Dedifferentiation. Am J Surg Pathol: March 1997; 21; pp 271-281