
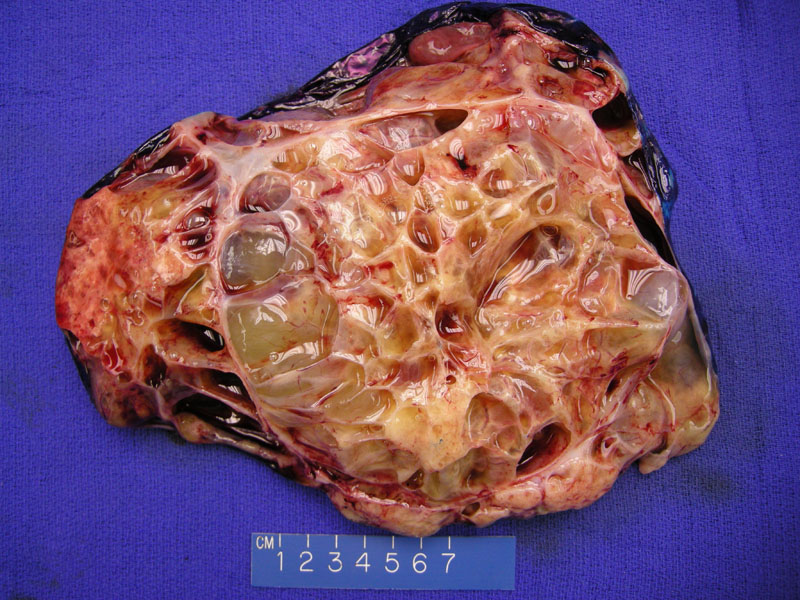
Grossly, the cut surface of the complex ovarian mass demonstrates multiloculated thin-walled cysts containing abundant mucin. Image
){kind=link}
Normal ovarian stroma is seen on the upper right and a metastatic colonic gland is seen on the lower left. Hemorrhage lies between the two.
){kind=link}
The lesion consists of complex cribriforming glands with central 'dirty' necrosis.
){kind=link}
A corpus albicans is seen in the upper image, with malignant glands from the colon arranged in a garland-like pattern (draping around the cystic space) in the bottom image.
){kind=link}
Cellular ovarian stroma is infiltrated by variably sized glands and although difficult to see on H&E, some single malignant cells.
){kind=link}
Reactive surface cells show cytokeratin 7, while the metastatic colonic glands are negative. Although negative CK7 staining is the classic pattern, it should be pointed out that both primary ovarian mucinous tumors and metastatic mucinous carcinomas of upper intestinal tract origin are capable of showing keratin 7 expression.5
){kind=link}
Cytoplasmic cytokeratin 20 is variably strong in the glands. Metastatic mucinous carcinomas of lower gastrointestinal tract origin (colon, rectum, and appendix) frequently express CK 20, as do some metastatic mucinous carcinomas of upper gastrointestinal tract origin (stomach and pancreaticobiliary tract). It is important to note that primary ovarian mucinous tumors demonstrate immunoreactivity for CK20, albeit staining is usually focal and weak.5
){kind=link}
Larger and smaller glands stain uniformly strong for nuclear CDX-2. While virtually all primary and metastatic colonic carcinomas show diffuse (3+) strong CDX2 reactivity, by contrast ovarian serous and endometrioid tumors are CDX2 negative. Of note, many ovarian mucinous carcinomas may show 1+ or 2+ immunoreactivity.4 Among other adenocarcinoma, CDX2 has been show to be expressed in metastatic appendiceal, pancreaticobiliary, and gastric carcinomas.5
){kind=link}
Estrogen receptor staining is negative in the glands. Some ovarian stromal cells show positivity. Interestingly, nuclear ER-beta immunoreactivity has been reported in >10% of the malignant cells and is almost always associated with cytoplasmic immunoreactivity.6
){kind=link}
All segments of the large bowel can give rise to a primary colorectal carcinoma that metastasize to the ovaries, but the most common location is the rectosigmoid. Some patients present with adnexal masses subsequent to the diagnosis of primary colon cancer. In other patients, however, adnexal masses may be the initial presentation, thus posing a diagnostic challenge to the surgical pathologist, especially during a frozen section.1
Microscopically, the metastatic glands range from small and tubular to large and dilated with complex cribriforming architecture. The lining cells are columnar and stratified, usually lacking mucin and thus appearing endometrioid. The cells also display prominent atypia and brisk mitotic activity. Occasionally, the glands can exhibit well-differentiated mucinous cells and produce copious mucin (colloid carcinoma). Characteristically, necrotic debris (dirty necrosis) fills the cystic or glandular lumen.1,2
Lee and Young compared and contrasted histologic features of 25 primary and 25 metastatic tumors of the ovary. Features that favored metastasis include (1) bilaterality, (2) microscopic surface involvement by epithelial cells (surface implants) and (3) an infiltrative pattern of stromal invasion. Features that favored a primary origin include (1) an "expansile" pattern of invasion and (2) a complex papillary pattern. Other features that were helpful distinguishing features (but less frequently present) were also noted in this interesting study.3
IHC will be extremely helpful in differentiating between a primary versus metastatic process. Metastatic colorectal cancers will be CK20+, CK7-, CEA+ and CA-125 negative. Primary ovarian endometrioid adenocarcionmas are CK7+, CK20-, CEA and CA-125 positive. Note, however, that this panel of stains may be less helpful in distinguishing a metastatic colon cancer from a primary mucinous ovarian carcinomas as the latter may exhibit intestinal differentiation (focal positivity for CK20 and CEA); furthermore, some mucinous colonic adenocarcinomas (as well as right-sided and rectal adenocarcinomas) exhibit focal CK7 positivity. As always, IHC results must be interpreted in the context of morphologic and clinical data.1
As a side note, some unfortunate individuals (ie. Lynch syndrome II) may have co-existing synchronous primary tumors of the colon and ovary.
Most common from the 5th to 9th decade. Patients typically present with abdominal pain and an ovarian mass seen on imaging. Up to 10% of women with intestinal cancer have ovarian metastases.1,2 Approximately two-thirds are bilateral. Grossly, smaller tumors may be solid and large tumors may have a cystic component that contains necrotic material, mucin, blood or clear fluid.
Treatment is as for colonic adenocarcinoma. The surgical oophorectomy should be part of appropriate and debulking procedure. To ensure the appropriate surgeons are present during the debulking procedure it is important to adequately work up any patients with hematochezia or melena before proceeding to the OR.
Colonic adenocarcinomas presenting as an ovarian metastasis are already stage IV and associated with a very poor prognosis.
• Ovary : Endometrioid Adenocarcinoma
• Ovary : Mucinous Cystadenocarcinoma (Expansile Type)
1 Nucci MR, Oliva Esther. Gynecologic Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier: 2009: 540-545, 684-6.
2 Mills SE, ed. Sternberg's Diagnostic Surgical Pathology.4th Ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2004: 2625.
3 Lee KR, Young RH. The distinction between primary and metastatic mucinous carcinomas of the ovary: gross and histologic findings in 50 cases. Am J Surg Pathol. 2003 Mar;27(3):281-92.
4 Groisman GM, Meir A, Sabo E.The value of Cdx2 immunostaining in differentiating primary ovarian carcinomas from colonic carcinomas metastatic to the ovaries. Int J Gynecol Pathol. 2004 Jan;23(1):52-7.
5 Vang R,et al. Immunohistochemical expression of CDX2 in primary ovarian mucinous tumors and metastatic mucinous carcinomas involving the ovary: comparison with CK20 and correlation with coordinate expression of CK7.Mod Pathol. 2006 Nov;19(11):1421-8.
6 Witte D, Chirala M, Younes A, Li Y, Younes M. Estrogen receptor beta is expressed in human colorectal adenocarcinoma.Hum Pathol. 2001 Sep;32(9):940-4.