
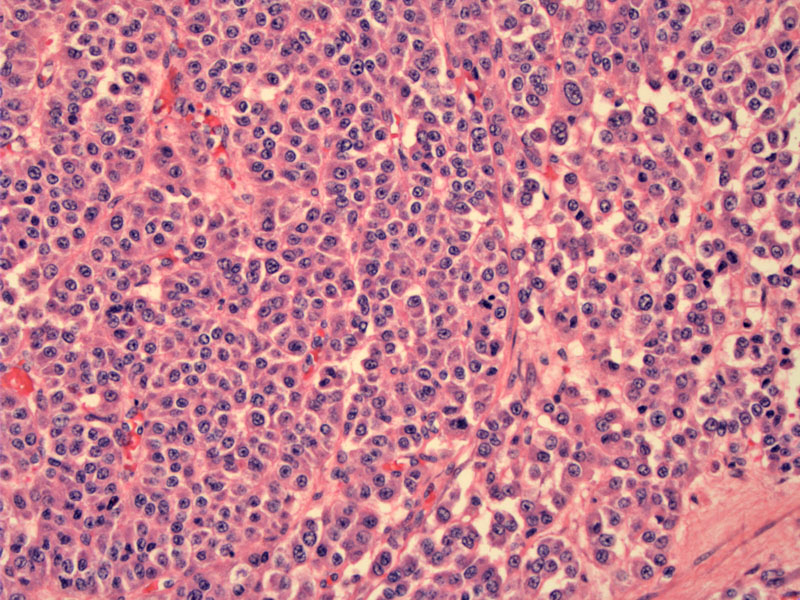
Polygonal cells with abundant eosinophilic cytoplasm grow in diffuse sheets. The nuclei are centrally placed with small nucleoli.
){kind=link}
These pink polygonal cells resemble Leydig cells, however, Reinke crystals are not found in the cytoplasm.
){kind=link}
Some cells contain clear or vacuolated cytoplasm, resembling adrenal cortical cells. The nuclei are quite vesicular here.
){kind=link}
A different case demonstrates Leydig-like cells with a peculiar sclerosing background.
){kind=link}
Another case shows a network of thin-walled compressed vessels. Note the prominent nucleoli in these steroid cells.
){kind=link}
At lower power, a diffuse sheet of monotonous cells can be appreciated. Note that the cytoplasm of the lesional cells ranges from granular and eosinophilic to pale and vacuolated.
){kind=link}
Yet another case demonstrates polygonal eosinophilic cells in diffuse sheets. There some mild atypia present in focal areas.
){kind=link}
Steroid cell tumor NOS (not otherwise specified) is a heterogenous group of ovarian stromal tumors that currently can not be further subclassified. Grossly, the tumors are well-circumscribed and solid ranging from 1 cm to 20 cm in diameter. The cut surface is tan, yellow or orange and occasionally tumors exhibit areas of necrosis and hemorrhage.
Microscopically, two populations of cells in varying proportions are seen: (1) Leydig-like cells resembling Leydig cells, but lacking the distinctive Reinke crystals of true Leydig cells. The cells are round or polygonal with abundant eosinophilic or sometimes vacuolated cytoplasm. The nuclei are round, centrally located with a prominent nucleoli; (2) Adrenal cortical-like cells are round or polygonal with abundant pale, clear and vacuolated cytoplasm. The nuclei are vesicular with small conspicuous nucleoli.1,2
Features associated with clinical malignancy include: (1) size greater than 7 cm; (2) hemorrhage or necrosis; (3) greater than 2 MF/10 HPF; (4) moderate or market nuclear pleomorphism.
Steroid cell tumors are immunoreactive for inhibin and calretinin. Interestingly, the tumors also stain for S100, Melan-A and HBM-45 in many cases, but the related marker MART-1 is negative.
Average age of presentation is 45 years old, but may be seen in a wide age range (2-80). Most of the tumors secrete enough androgens to cause virilization or hirsutism. Serum levels of testosterone and urinary 17-ketosteroids are usually elevated in these patients. A minor subset of patients have estrogenic manifestations such as postmenopausal bleeding or Cushing syndrome due to cortisol secretion by the tumor cells.
As most of these unilateral, younger patients with Stage IA tumors can undergo unilateral salpingo-oopherectomy to preserve fertility. For older patients without fertility concerns, bilateral salpingo-oopherectomy and hysterectomy would be advised.
Extraovarian spread is detected in 20% of cases at the time of diagnosis. Those who present with Cushing syndrome tend to present with advanced disease (extensive extraovarian spread). Approximately 20% of patients experience recurrence more than 5 years later.1,2
1 Nucci MR, Oliva Esther. Gynecologic Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier: 2009: 495-498.
2 Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 601.