
Sheets of malignant, enlarged monocytoid-appearing histiocytes are present with eosinophilic cytoplasm.
){kind=link}
At higher power, moderate atypia is apparent.
){kind=link}
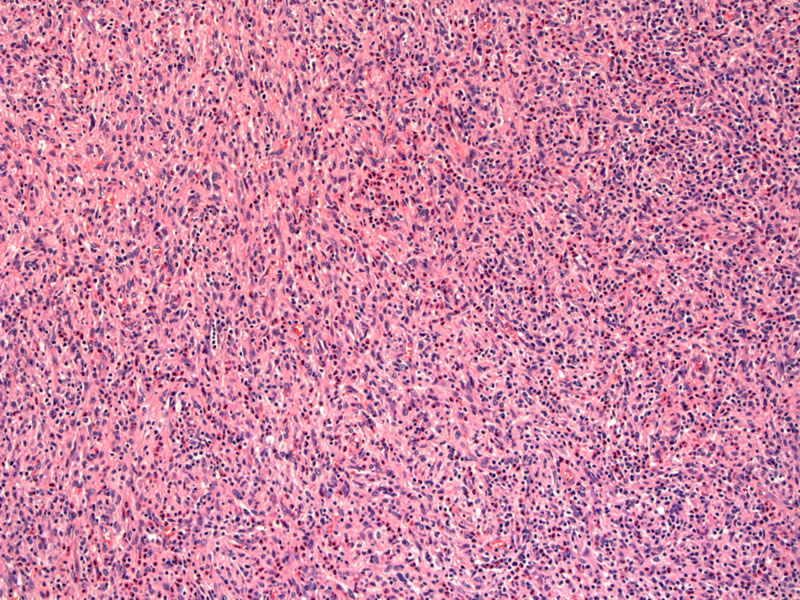
This image shows a mixed lymphoid infiltrate present in the background, with prominent eosinophils.
){kind=link}
Though the malignant histiocytes are more often rounded in shape, they sometimes can show a spindled morphology, as shown in this image.
){kind=link}
Histiocytic markers are strongly positive in this neoplasm. This image shows reactivity to CD68.
){kind=link}
CD163, another histiocytic marker, shows more diffuse staining.
){kind=link}
Lysozyme, another histiocytic marker, is positive
){kind=link}
CD4, a marker of normal T-lymphocytes, is also often positive.
){kind=link}
This rare neoplasm is composed of mature histiocytes and occurs most commonly in extranodal sites such as the gastrointestinal system, skin and soft tissues. Histocytic neoplasms such as this one can arise from pluripotential germ cells. This may be the reason why these tumors can be seen in patients with a concurrent mediastinal germ cell tumor, such as teratoma. This tumor can also be precede or present in association with malignant lymphoma, myelodysplasia or leukemia. Should a patient have the rare presentation of multiple sites of involvement, this is referred to as 'Malignant histiocytosis'. Not to be confused with malignant histiocytosis X, which is an older name for the WHO entity called Langerhans cell sarcoma.
Histologically, the cells are large, non-cohesive and have vesicular chromatin with variable atypia. Occasional multinucleated tumor cells and/or hemophagocytosis can be seen. Background reactive cells such as neutrophils and eosinophils are present in varying amounts.
Immunohistochemistry is essential to rule out other malignancies such as melanoma and large cell lymphoma. The tumor cells stain for histiocytic markers such as CD163, CD68 and lysozyme. Langerhans cell markers such as CD1a, myeloid markers such as CD33, and melanoma cell markers such as mean-A are negative. Be wary of S-100: weak or focal staining may be present in histiocytic sarcoma, however the diffuse positivity characteristic of most melanomas is not present.
Ultrastructurally, birbeck granules are not seen. (Tennis-racket shaped structures found in Langerhans cells)
Histiocytic sarcomas are rare and have a wide age range, though most occur in adults. The majority of cases arise in extranodal sites, especially in the intestinal tract. For this reason, patients may present with intestinal obstruction. Skin manifestations may vary from a simple rash to numerous tumor masses on the trunk and extremities. Often patients present with complaints of fever and weight loss and imaging studies may reveal hepatosplenomegaly and/or bony lytic lesions. Sequestration due to hepatosplenomegaly may result in CBC values showing pancytopenia.
Treatment consists of chemotherapy.
The prognosis is poor, both due to the aggressive nature of the neoplasm and the frequent high stage presentation.
• Nasopharynx : Langerhans Cell Histiocytosis
• Liver : Hepatocellular Carcinoma
• Thyroid : Diffuse Large B-Cell Lymphoma
• Salivary Gland : Large Cell Lymphoma
1 Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Vardiman J, WHO Classification of Hematopoeitic and Lymphoid Tissues 4th Ed. WHO Press; 2008: pp 356-357.
2 Sonneveld P, van Lom K, Kappers-Klunne M, Prins ME, Abels J. Clinicopathological diagnosis and treatment of malignant histiocytosis. Br J Haematol. 1990 Aug;75(4):511-6.