
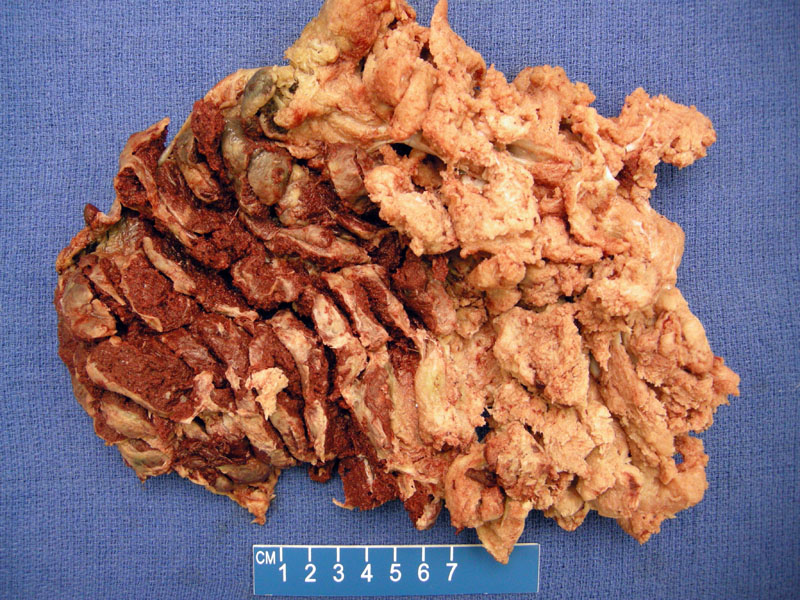
Note the vascular portion (left) and the pale portion (right) of this twin placenta. The vascular portion belongs to the recipient twin and the pale portion belongs to the donor twin.
 can be appreciated.', 'micro', '')){kind=link}
Twin-to-twin transfusion syndrome (TTTS) is caused by an unidirectional arteriovenous anastomoses in the monochorionic twin placenta leading to unequal sharing of blood between twins. Vascular anastomoses occur in monochorionic twin placentas and only rarely in dichorionic placentas. There may be bi-directional arterial-venous anastomoses, arterial-arterial and venous-venous connections. In instances where a large variety of anastomoses exist, the blood flow in the placenta will be balanced, and both twins will receive blood and nutrients.1,2
However, if AV anastomoses are not 'balanced out' by other anastomoses, unidirectional blood flow occurs from the donor twin to the recipient twin. The donor twin will exhibit oligohydramnios whereas the recipient twin will exhibit polyhydramnios. The donor twin will usually be smaller and anemic, and the recipient twin is usually plethoric and large. The size difference is most striking in the heart.
Frequency of TTTS is estimated between 5%-30% of monochorionic twin pregnancies. The condition is usually first detected as an imbalance in amniotic fluid. Subsequent growth discrepancies may later develop. As mentioned above, the severity can range from mild to severe. When the condition is diagnosed before 28 weeks, overall survival of the pregnancy is approximately 21%. The donor suffers from a lack of nutrients and the recipient suffers from congestive heart failure.1
Obliteration of the vascular connections by fetoscopic laser ablation(in utero) may be attempted. Other treatments include amnioreduction or the creation of a window between the two amniotic sacs. Delivery is effected once critical levels of fetal compromise are reached- typically preterm.
The donor twin usually fares better than the recipient. Other prognostic considerations include amnionicity and prematurity at delivery.
1 Baergen RN. Manual of Benirschke and Kaufmann's Plathology of the Human Placenta. New York, NY: Springer; 2005: 163-6.
2 Mills SE, ed. Sternberg's Diagnostic Surgical Pathology.4th Ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2004: 2315-16.