System: Skin: Epithelial: Indeterminant: Porokeratosis

System: Skin: Epithelial: Indeterminant: Porokeratosis

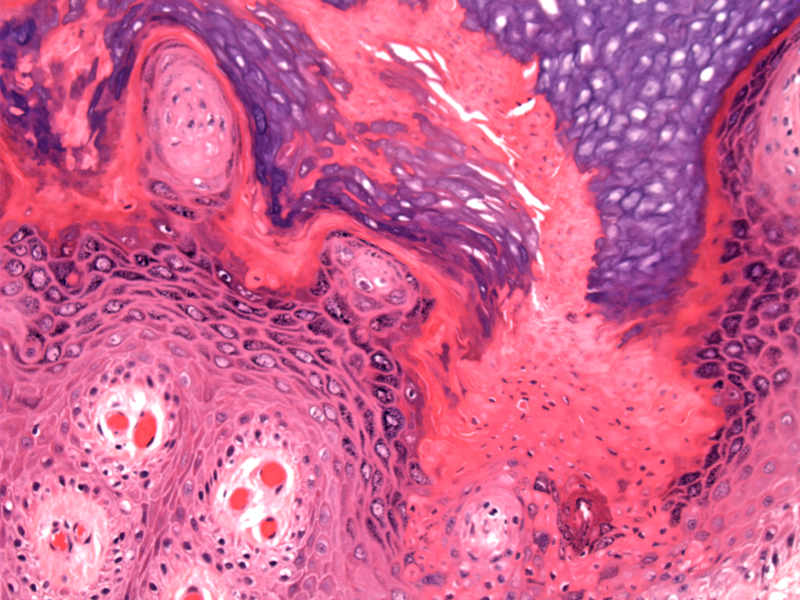
Case 1: The key diagnostic feature of porokeratosis is cornoid lamella, which is a column of parakeratosis overlying hypogranulosis and dyskeratosis. The columns of cornoid lamella often slant or lean toward the center of the lesion.
A pink column of cornoid lamella is seen to the right. The epidermis in the central portion of the lesion may be hyperplastic, normal or atrophic.
Case 2: A low power view of the column of parakeratosis.
Note the diminished granular layer giving rise to the parakeratosis.
Another example Image
2 Image
Porokeratosis is a disorder of keratinization characterized by the formation of one or more atropic patches surrounded by a raised border of cornoid lamella, a key diagnostic feature of this entity. The pathogenesis of these lesions are still not entirely known, but there is an inherited predisposition and immune host response plays a role.
Five clinical variants of porokeratosis have been described (McKee, Spencer):
Clinically, an annular lesion with a "threadlike elevated border" is seen (Rapini). This threadlike border corresponds to the cornoid lamellae seen histologically.
Treatment depends on the type of porokeratosis and includes topical medications such as 5-Fluorouracil. Oral retinoids are sometimes used. For lesions with malignant transformation, surgical excision will be necessary.
→Although cornoid lamellae can be seen in other conditions (e.g. actinic keratosis), for an exam, think porokeratosis.
McKee PH. Pathology of the Skin with Clinical Correlations 2nd Ed. London, UK: Mosby-Wolfe; 1996: 2.20-2.22.
Spencer, LV. Porokeratosis: eMedicine. Last updated on 8/3/09. Available at emedicine.medscape.com/article/1059123-overview

){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}