
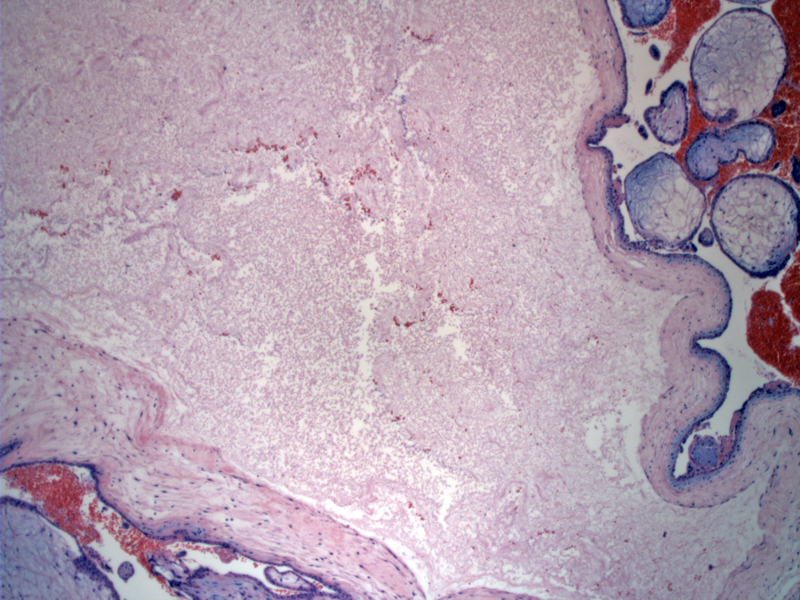
Dilated large hydropic villi with avascular central cistern are seen in some of the villi.
){kind=link}
Other villi appear normal, and some of the non-hydropic villi may even be fibrotic. Also, there is no significant trophoblastic proliferation.
){kind=link}
This particular case demonstrates more trophoblastic proliferation, although it is still irregular and patchy. The trophoblasts exhibit mild cytologic atypia.
){kind=link}
Although this is a 'soft' feature, the villi in partial moles often have a scalloped and undulating border, versus a broad and bulbous contour of complete moles.
){kind=link}
p57 stains cytotrophoblasts and maternal decidualized stromal cells.
){kind=link}
This is a different case from a patient with abnormally elevated b-HCG and tissue which proved to be triploid. Note that the possibility of an early normal pregnancy might easily be entertained.
){kind=link}
Other areas of this tissue are more suggestive of molar pregnancy.
){kind=link}
In partial moles, only some of the villi are edematous whereas in complete moles, all the villi are edematous. Similar complete moles, trophoblastic proliferation is also random and circumferential, but in partial moles,the trophoblastic proliferation tends to be focal. This is in contrast to a hydropic abortus, where the trophoblastic proliferation is polarized at the anchoring villi. Fetal parts may be seen in partial moles, and unless the complete mole is paired with a twin pregnancy, fetal parts are never seen in complete moles.
Other subtle differences between partial and complete moles include (1) irregular and scalloped border with deep indurations (versus a broad and bulbous contour in complete molar villi; (2) as a consequence of the deep infoldings, one may see trophoblastic 'inclusions' in the villi from tangential sectioning; (3) the implantation site is trophoblastic cells only exhibit minimal atypia compared to the exaggerated implanation site with prominent cytologic atypia in complete moles.1,2
Partial moles are generally triploid as a result of fertilization of a normal egg by one or two sperm. If it is a single sperm, the sperm undergoes androgenesis (division) to result in a triploid set of DNA. Two-third of cases are 69XXY, and less often 69XXX or 69XYY. Since maternal DNA is present, p57 IHC will stain some of the cytotrophoblastic cells.
Unlike in complete moles, there are usually enough functional villi present to support embryologic development in partial moles. The uterus tends to be small for gestational age and serum hCG are in the low or normal range (compared to uterus large for dates and extremely high titers seen in complete moles). Patients typically present with vaginal bleeding and are diagnosed on ultrasound, as with complete moles.1,2
Treatment is by uterine evacuation via dilation and curettage.
The risk of persistent gestational trophoblastic disease is present in the setting of partial moles, though less than with complete moles.
• Placenta : Hydropic Products of Conception
• Placenta : Complete Molar Pregnancy
1 Kumar V, Abbas AK, Fausto N. Robbins and Cotran Pathologic Basis of Disease. 7th Ed. Philadelphia, PA: Elsevier; 2005: 1110-1113.
2 Mazur MT, Kurman RJ. Diagnosis of Endometrial Biopsies and Curettings. New York, NY: Springer; 2005: 67-74.