
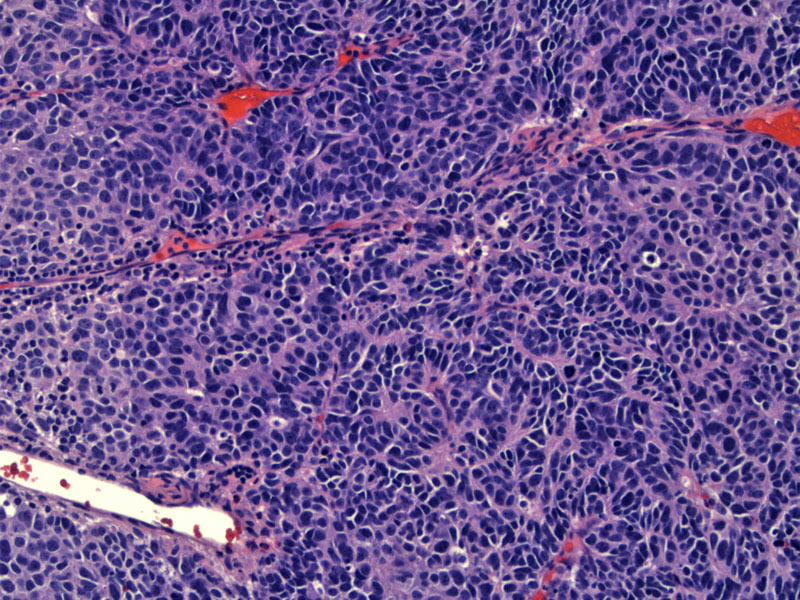
Large cell neuroendocrine tumors are defined by their neuroendocrine morphology which includes organoid nesting, palisading, trabecular pattern and rosette like structures. In this image, there is a combination of nesting and trabecular patterns.
){kind=link}
There are often large zones of necrosis.
){kind=link}
The malignant cells exhibit abundant cytoplasm (when compared to small cell carcinoma) with frequent conspicuous nuclei.
){kind=link}
A mitotic count of 11 or more mitoses per 10 high power fields is the main criterion separating large cell neuroendocrine carcinoma and small cell carcinoma from atypical carcinoid.
){kind=link}
Neuroendocrine markers such as CD56 (NCAM) are positive.
){kind=link}
Corresponding synaptophysin is positive. Large cell neuroendocrine carcinomas express most neuroendocrine markers (chromogranin, neuron specific enolase, synaptophysin, somatostatin) but are negative for the high molecular weight cytokeratins typically seen in small cell carcinoma (Jiang. About half show TTF-1 reactivity.
){kind=link}
A different case clearly demonstrates numerous mitotic figures can be appreciated in this image.
){kind=link}
This other example shows broad trabeculae as well as the cytological features of this tumor.
){kind=link}
Central necrosis can often be found within tumor nests.
){kind=link}
Yet another example shows brisk intervening lymphoplasmacytic inflammation.
){kind=link}
Large cell neuroendocrine carcinoma (LCNEC) is currently considered a variant of large cell carcinoma, but with neuroendocrine features. These tumors have been termed "intermediately differentiated neuroendocarcine carcinoma", or "large cell carcinoma of the lung with neuroendocrine differentiation".
Microcopically, the features of LCNEC are: (1) large cell size compared to small cell carcinoma, polygonal in shape with abundant cytoplasm and vesicular nuclear chromatin with conspicuous nucleoli; (2) neuroendocrine architecture such as rosette formation, palisading or trabeculae; (3) mitotic activity greater than 11 mitoses per 10 hpf; (4) prominent zones of necrosis and (5) positivity with neuroendocrine markers such as chromogranin, synaptophysin and NCAM/CD56 (Zander).
LCNEC are uncommon, comprising 3% of lung tumors (Zander). The median age at presentation is 65 (Takei). Clinical features of LCNEC are hybrids of adenocarcinoma and small cell carcinoma. For example, like small cell carcinoma, most patients are male with a strong smoking history, but like adenocarcinomas, they more frequently present with peripheral tumors but can be centrally located. Patients usually present with symptoms similar to NSCLCs and usually lack paraneoplastic syndromes, but again with similarity fo small cell cardinoma, Eaton-Lambert syndrome have been documented in LCNEC patients (Leslie)
Because of the relative rarity of this tumor, optimal therapy remains uncertain, but most patients with early stage LCNEC are surgically treated. Surgery alone is not sufficient, however, even in early stage disease, so perioperative chemotherapy is usually also advised.
This is regarded as an aggressive tumor that behaves similarly to small cell carcinoma. In one study, these two tumor types showed the same behavior stage for stage.
Leslie KO, Wick MR. Practical Pulmonary Pathology. Philadelphia, PA: Elvesier; 2005: pAGE 444-6.
Jiang SX et al. Large cell neuroendocrine carcinoma of the lung: a histologic and immunohistochemical study of 22 cases, Am J Surg Pathol 22 (1998), pp. 526–537.
Takei H et al. Large cell neuroendocrine carcinoma of the lung: a clinicopathologic study of eighty seven cases, J Thorac Cardiovasc Surg 124 (2002), pp. 285–292.
Zander DS, Farver CF. Pulmonary Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elvesier; 2008: 570-5.