System: Skin: Vascular: Benign: Papillary Endothelial Hyperplasia


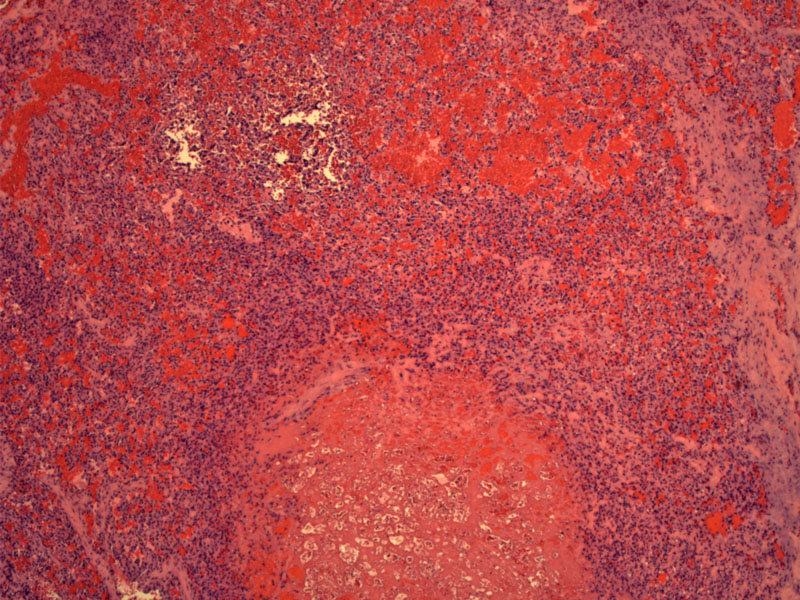
Case 1: A thrombus formation
Part of vascular wall shown on right so you can tell it arises intravascularly; the lesion is well circumscribed, lacking an infiltrative border.
Case 2: Vascular channels are formed by papillary structures. The papillary cores are hypocellular, hyalinized and occasionally contain small vessels.
Papillary endothelial ingrowth (bottom half) results in a papillae fusion to form loosely anastomatic appearance.
Papillae are composed of hypocellular hyalinized cores lined by bland endothelial cells; there is no atypia or mitotic activity.
Close up of the papillae in association with a vascular wall. Although most papillae appear to be detached from the vessel wall, some are indeed attached to it.
Papillary endothelial hyperplasia (PEH) is a benign reactive proliferation of endothelial cells arising in an organized thrombus. It can occur in three settings: (1) primary form (most common) -- arises within a dilated blood vessel; (2) secondary form -- arising within pre-existing conditions such as a hemangioma or varices; (3) rarely, in association with a hematoma in an extravascular location (Konstaninos).
Histologically, primary PEH begins within a thrombosed vessel, and thus, is composed of a well-circumscribed papillary proliferation vessels. These small vessels are lined by bland, attenuated endothelial cells. Secondary PEH would have the same features, but will be arising within a secondary lesion such as a hemangioma.
It is important to be aware of this condition because it can be confused with angiosarcoma. Both lesions may form anastamosing channels, but in angiosarcoma, the endothelial cells are atypical and mitotically active. Of note, spindle cell hemangioma can also arise within a vessel, but spindle cell hemangioma is characterized by features of cavernous hemagioma and Kaposi-like spindle cells forming slit-like spaces (Folpe).
In the primary type lesion (arising within a blood vessel), it presents as a painless bluish nodule, typically on the finger or the head and neck region of young adults.
Cured by simple excision in primary forms, and by treating the underlying condition in the secondary forms.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 41-2.
Folpe AL, Inwards CY. Bone and Soft Tissue Pathology: Foundations in Diagnostic Pathology Philadelphia, PA: Elsevier; 2010: 164-5.
Konstantinos T, Ioannis GK, Papanicolaou SI. Intravascular papillary endothelial hyperplasia of the oral soft tissues: report of 18 cases and review of the literature. J Oral Maxillofac Surg 1994;52:1263–1268.
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}