
With the exception of appendiceal carcinoids where the tumor may appear as a bulbous mass that obliterates the lumen, all other carcinoids in the GI tract are intramural or submucosal lesions that form a polpoid mass or plateau. The overlying mucosa can be intact or ulcerated. The tumors are generally less than 3 cm in greatest dimension.
. ', 'gross', '')){kind=link}
Sectioning an ileum carcinoid (from a different case) reveals a very solid yellow-tan mass. The firmness is a result of extensive desmoplasia. If the tumor invades through the bowel wall into the mesentery (as ileal carcinoids tend to do), prominent fibrosis can occur and lead to kinking or angulation of the intestines. Not surprisingly, intestinal obstruction is a common complication.
){kind=link}
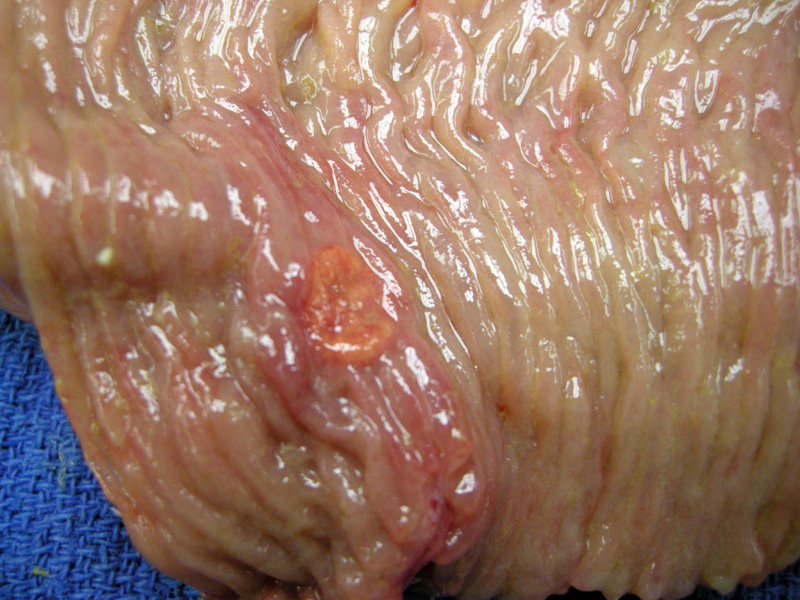
A different case demonstrates a polypoid carcinoid located near the ileocecal valve, the preferred site for jejunoileal carcinoids.
){kind=link}
Normal ileum is seen overlying the carcinoid tumor. These lesions are commonly arranged in nests (as demonstrated in this image). Other patterns include trabecular, glandular, cribriform or solid.
){kind=link}
A higher power demonstrate nests of monomorphic tumor cells with centrally placed round nuclei and pink granular cytoplasm. The nests are surrounded by a network of fibrovascular stroma.
){kind=link}
A salt and pepper chromatin pattern is typical of neuroendocrine tumors.
){kind=link}
Carcinoids are reactive with most neuroendocrine markers such as synaptophysin, chromogranin, NSE and PGP 9.5. In this image, a different case of ileal carcinoid demonstrate strong staining for synaptophysin.
){kind=link}
The gastrointestinal tract contain the most number of neuroendocrine cells in the body, thus not surprisingly, a significant proportion of neuroendocrine neoplasms arise from various sites along the GI tract. The other frequent site for neuroendocrine tumors is the lung. The classification of these tumors is currently a work in progress. Indolent tumors are variably termed "carcinoids" or "well-differentiated neuroendocrine tumors". More aggressive tumors are termed "poorly differentiated neuroendocrine carcinomas" or simply "neuroendocrine carcinomas".1
Admittedly, these terms are confusing and suboptimal. The classification of neuroendocrine tumors in the lung have made more progress, with current favored terms of typical carcinoid (low-grade), atypical carcinoid (high-grade) and large cell neuroendocrine carcinoma (high-grade) and small cell carcinoma (high-grade). Large cell neuroendocrine carcinoma and small cell carcinoma also exist in the GI tract as high-grade lesions. Therefore, it may be helpful to keep in mind the classification of neuroendocrine tumors of the lung when thinking of the GI tract.
For this discussion, I will use the term carcinoid to refer to neuroendocrine tumors in the GI tract that are well-differentiated. The term carcinoid is unlikely to leave the pathology lexicon, therefore, it would be prudent to understand its history and its current usage.
Another note on terminology that may be helpful is that tumors that are functional and secrete biologically active peptide hormones are named after the type of hormone secreted (ie. gastrinoma, glucagonoma, somatostatinoma). On the other hand, tumors that are endocrinologically silent but demonstrate a predominant secretory product immunohistochemically are designated as ECL-, G-, EC- neuroendocrine tumors. ECL stands for enterochromaffin-like cells that secrete histamine, G cell stands for gastrin-producing G cells, EC stands for enterochromaffin cells that produce serotonin and so on. 1
As all carcinoid tumors have malignant potential the terms "benign" and "malignant" are poor terms to describe these tumors. Higher grade neuroendocrine tumors may demonstrate necrosis and increased number of mitotic figures, however, one must remember than even bland appearing carcinoids can metastasize. Therefore, one must rely on a constellation of features such as tumor size (greater than 2 cm), extent of intramural invasion, anatomic site in order to make an educated guess regarding tumor behavior.
The appendix is the most commonly affected site, followed by the small intestine, rectum, stomach and colon. Appendiceal and rectal carcinoids very rarely metastasize despite extensive intramural invasion. In comparison, the majoriy of neuroendocrine tumors in the duodenum, ileum and colon are metastatic at the time of presentation. As for gastric neuroendocrine tumors, a subset are metastatic. Tumors in the stomach and ileum are frequently multicentric, but those arising elsewhere in the GI tract tend to be solitary.2
Jejunoileum carcinoids are multicentric in ~30% of cases. 70% occur in the ileum (with the majority in the ileocecal valve), 11% in the jejunum and ~3% in Meckel's diverticulum.3
Patients may present with abdominal pain as a result of intestinal obstruction, and up to 18% may present with the typical carcinoid syndrome, as the tumor may elaborate serotonin and metastasize to the liver.2 Note that normally, GI carcinoids do not cause the carcinoid syndrome because the liver will degrade the peptide hormones.
1 Dayal Y. Neuroendocrine Tumors of the Gastrointestinal Tract. Pathology Case Reviews. 2006;11:268-281.
2 Kumar V, Abbas AK, Fausto N. Robbins and Cotran Pathologic Basis of Disease. 7th Ed. Philadelphia, PA: Elsevier; 2005: 866-868.
3 Hamilton SR, Aaltonen LA. Eds. Tumours of the Digestive System: World Health Organization Classification of Tumours Lyon: IARC Press; 2000: pg 80-82.