
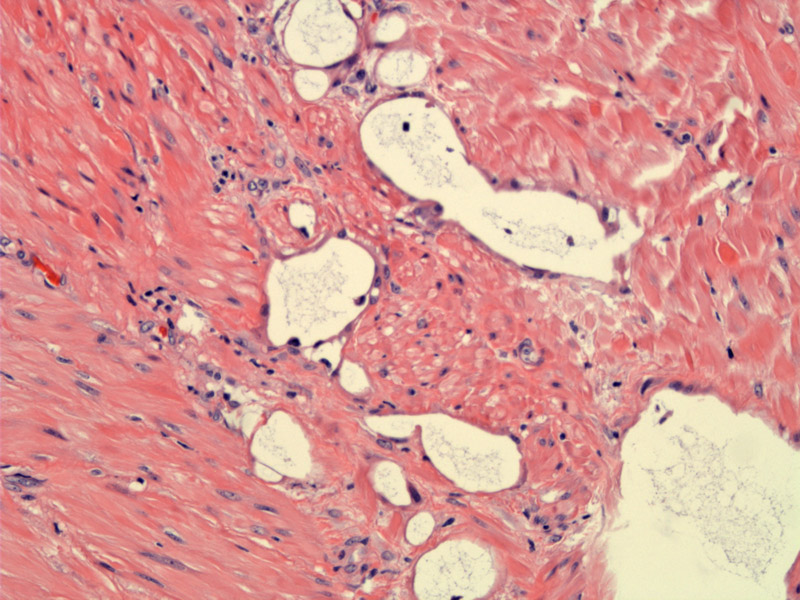
Variably-sized pseudovascular structures are separated by bands of smooth muscle.
){kind=link}
Attenuated mesothelial cells line these pseudovascular structures. The glands have an infiltrative growth pattern but lack atypia.
){kind=link}
The mesothelial cells lining the pseudovascular structures demonstrate mesothelial markers such as calretinin, HMBE-1 and WT-1. In this image, the lining cells are positive for calretinin. This marker is present in virtually all cases of adenomatoid tumor4 .
){kind=link}
The mesothelial cells are also strongly positive for keratin 7. Lymphoangiomas (high on the differential) are not positive for cytokeratins.2
){kind=link}
Another tumor demonstrates smaller caliber structures dissecting in an infiltrative manner. These pseudovascular structures permeate through bands of smooth muscle.
){kind=link}
Adenomatoid tumors originate from the serosal mesothelium. They are most commonly in a subserosal location and most are less than 5 cm. However, they may become quite large and extend toward the endometrium.1,2
On gross inspection, adenomatoid tumors may mimic a leiomyoma. However, adenomatoid tumors are less circumscribed than leiomyomas and are typically poorly-demarcated from the surrounding myometrium. Microscopically, there is proliferation of pseudovascular spaces lined by attenuated epithelium. The tubular structures are separated by bands of smooth muscle. These tumor were often mistaken for lymphangiomas in the past, however, ultrastructural and immunohistochemical studies have confirmed their mesothelial origin.
The cells lining the pseudovascular spaces are mesothelial cells that stain positively with keratin, calretinin, HMBE-1 and WT-1.1
Benign; usually an incidental finding.
1 Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 688.
2 Kurman RJ, Norris HJ, Wilkinson E. Tumors of the Cervix, Vagina and Vulva: Atlas of Tumor Pathology. Third Series Fascicle 4. Washington DC; AFIP: 1990: Section 6.6.
3 Sternberg SS, ed. Diagnostic Surgical Pathology.4th Ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2004: 2524.
4 Sangoi AR, McKenney JK, Schwartz EJ, Rouse RV, Longacre TA. Adenomatoid tumors of the female and male genital tracts: a clinicopathological and immunohistochemical study of 44 cases. Mod Pathol. 2009 Sep;22(9):1228-35.