
Endometrial polyps are comprised of a proliferation of benign stromal elements that entrap haphazardly placed benign endometrial glands.
){kind=link}
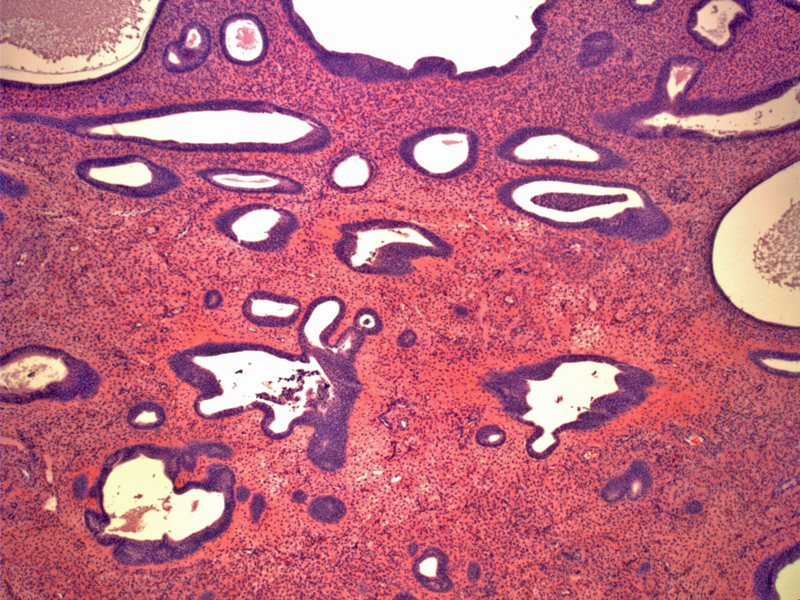
This atrophic polyp contains cystically dilated glands lined by attenuated epithelium.
){kind=link}
Another endometrial polyp demonstrates variably sized glands set in fibrotic stroma.
){kind=link}
Inactive appearing tubular glands are seen in this polyp. There is a proliferation of ectatic blood vessels as well.
){kind=link}
Endometrial polyps (EMP) are defined as "overgrowths of endometrial glands and stroma with blood vessels, sometimes containing uterine smooth muscle, which protrude into the uterine cavity"(Robboy). They can be sessile or pedunculated and occasionally, they can be seen at the external cervical os.
The diagnosis of endometrial polyp can be difficult in an endometrial curretage or biopsy specimen since the specimen is fragmented and loses its polypoid configuration. It has often been said that a helpful diagnostic feature is identification of a large fragment of endometrial tissue covered on three sides by surface epithelium. However, be cautious about this particular finding. Tangential removal of the regular endometrium during curretage may produce the same effect (Mazur).
Thus, it is best to rely the following key diagnostic features: (1) thick-walled vessels (2) fibrous or collagenous stroma (3) disordered placement of glands and (4) the glands may be 'out of sync' when compared to other endometrial glands.
Several types of endometrial polyps exist. The most common encountered polyp is the hyperplastic/proliferative polyp. The glands are haphazardly placed and resemble either the proliferative phase or hyperplasia (simple or complex) without atypia. It is helpful to look at other fragments of endometrium (not part of the polyp); the glands should either be proliferative or atrophic, or possibly secretory in a younger woman. In true hyperplasia of the endometrium, the hyperplasia should be diffuse and not confined to several fragments.
Atrophic polyps occur in postmenopausal women; the glands are lined with attenuated inactive epithelium. The stroma is often pale and fibrotic. Frequently, the glands may be dilated and thus called "cystic atrophic (senile) polyps".
Tamoxifen polyps (generally seen in women treated for breast cancer) are another variant, but are only encountered in a woman with a history of tamoxifen therapy. These polyps are larger, with edematous, myxoid or fibrous stroma. The glandular epithelium may show mucinous or clear cell change (Crum).
Similar to endocervical polyps, the peak incidence is in the 5th decade and presents as abnormal bleeding. Between 2%-5% harbor malignant neoplasia and these occur almost exclusively in postmenopausal women.
Endometrial polyps may be successfully treated medically using cyclic progestin-containing hormonal preparations or surgically with uterine curettage. Definitive treatment of endometrial polyps consists of a hysterectomy.
Benign endometrial polyps may recur if incompletely removed or may occur as separate new polyps. Prognosis of polyps with underlying malignancy depends on the cancer's stage.
Robboy SJ, Anderson MC, Russell P. Pathology of the Female Reproductive Tract. London, UK: Churchill Livingstone; 2002: 298-301.
Crum CP, Lee KR. Diagnostic Gynecologic and Obstetric Pathology. Philadelphia, PA: Elsevier; 2006: 461-5.
Mazur MT, Kurman RJ. Diagnosis of Endometrial Biopsies and Curettings. New York, NY: Springer; 2005: 134-5,163-70.
Nucci MR, Oliva Esther. Gynecologic Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier: 2009.