System: Genitourinary: Kidney: Medical: Dense Deposit Disease (MPGN II)

System: Genitourinary: Kidney: Medical: Dense Deposit Disease (MPGN II)

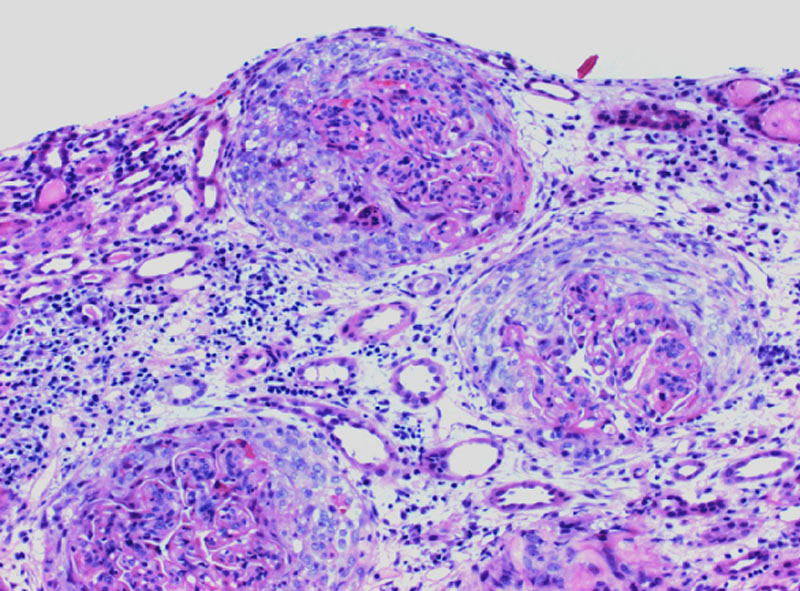
multiple injured glomeri show extensive involvement by cellular crescents, in a background of tubulointerstitial injury; crescents on early biopsy are a feature suggestive of a poor prognosis
Cellular crescent envelops a hypercellular glomerulus with closed capillary loops
Marked endocarpillary hypercellularlity composed of endocapillary proliferation and inflammatory cells. Thickened capillary walls are appreciated on this higher magnification
C3 shows a bright ribbon-like pattern outlining the glomerular basement membranes.
another case Image
thickened basement membrane Image
PAS nice Image
MPGN II can be associated with acquired partial lipodystrophy (APL)
M=F. Very rare.
Commonly affects children and young adults
Present with proteinuria and/or hematuria to varying degrees
often have hypocomplementemia
can screen for 'C3 nephritic factor' - an autoantibodies directed against C3bBb, the convertase of the alternative pathway (AP) of the complement cascade.
Distinguishing DDD from membranoproliferative glomerulonephritis type I may not be possible clinically since both are characterized by a nephrotic and/or nephritic clinical picture. In actuality, there aremarked differences in etiology and pathogenesis between type I membranoproliferative glomerulonephritis and dense deposit disease.
Spontaneous remission almost never occurs. The more likely outcome is chronic deterioration of renal function leading to renal failure in approximately half of patients within 10 yr (Appel). In others, rapid fluctuations in proteinuria occur with episodes of acute renal deterioration in the absence of obvious triggering events; others may manifest a more stable pattern for years despite persistent proteinuria (Appel).
Appel GB, et al. Membranoproliferative glomerulonephritis type II (dense deposit disease): an update. J Am Soc Nephrol. 2005 May;16(5):1392-403. Epub 2005 Mar 30.
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}