System: Head and Neck: Salivary Gland: Neoplastic: Epithelial-Myoepithelial Carcinoma

System: Head and Neck: Salivary Gland: Neoplastic: Epithelial-Myoepithelial Carcinoma

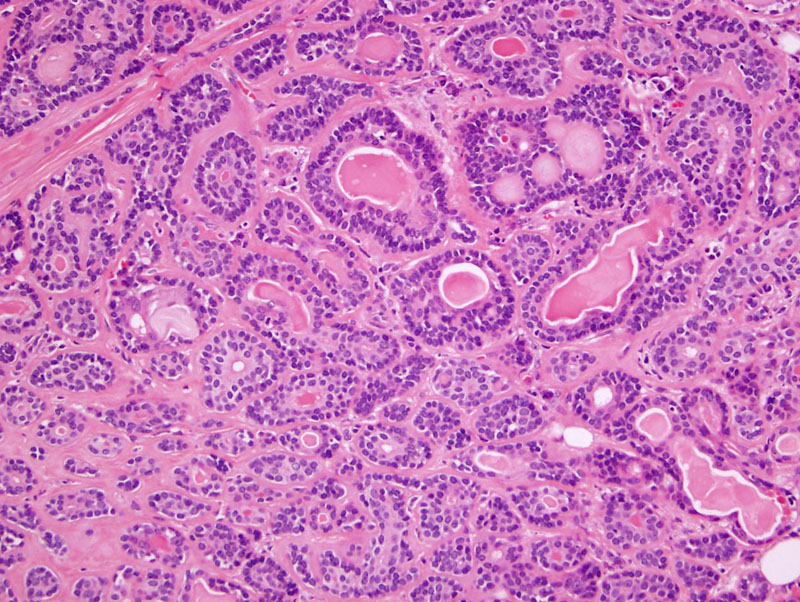
Case 1: A proliferation of ductal structures composed of an inner luminal-ductal layer and outer myoepithelial layer characterizes this tumor.
Case 2: This case appears to be myoepithelial cell predominent. The myoepithelial cells tend to be clear cytoplasm.
On higher power, the myoepithelial component with scattered luminal-ductal cells forming glandular/ductal structures can be appreciated.
Case 3: A different case that is more oncocytic and papillary.
Case 4: Here is the hyalinizing variant, with heavily sclerotic/hyalinized stroma between the ductal structures.
Perineural invasion is commonly seen in this tumor.
Case 5: The epithelial and myoepithelial cells can form solid sheets and trabeculae, with absent to minimal ductal structures.
Case 6: A great case with ductal-luminal cells and outer myoepithelial cells.
p63 can highlight the myoepithelial layer.
CAM 5.2 highlights luminal ductal cells.
SMA also highlights the myoepithelial layer.
Case 7: Despite a circumscribed gross appearance, these tumors have infiltrative margins as seen here.
This case also exhibits heavily hyalinized stroma with compressed cords of epithelial-myoepithelial cells.
Another area demonstrates neoplastic myoepithelial cells that are quite pleomorphic, with almost a sheet-like growth.
Epithelial-myoepithelial carcinoma (EMC) is a lesion composed of duct-like structures with morphology mimicking both inner ductal lining and outer myoepithelial cells. This is a rare lesion accounting for less than 1% of salivary gland tumors.
Grossly, EMC is well-circumscribed but non-encapsulated mass ranging from 2-8 cm in diameter with a lobulated and sometimes cystic cut surface. Note that although circumscribed grossly, these tumors tend to have infiltrative margins and perineural invasion.
Microscopically, EMC is comprised of duct-like structures lined by a double-layer. The inner luminal layer consist of a single layer of cuboidal or columnar cells with granular or eosinophilic cytoplasm. The outer myopeithelial layer consists of a single or multiple layers of cells with clear glycogenated cytoplasm (Thompson).
The ductal structures can form broad sheets, making the diagnosis difficult. Two variants have been described, the hyalinzing variant in which the stroma is sclerotic, and the clear cell or ductal poor variant, in which the luminal ductal cells are sparse or absent.
These tumors are usually seen in older adults and there is a female preponderance. In a study of 61 cases, the mean age was 60.9 years, with a female to male ratio of 1.5:1 -- the most common sites were parotid (62.1%), sinonasal mucoserous glands (10.3%), palate (8.6%), and submandibular gland (8.6%)(Seethala).
EMC typically presents as a slowly enlarging, painless mass in the parotid gland but may also be seen less frequently in minor salivary glands as ulcerated or submucosal nodules.
Treatment for EMC is parotidectomy with facial nerve preservation and lymphadenectomy if metastasis are diagnosed. The role of adjuvant radiation therapy is not well established, however, like most malignant lesions, it is reserved for patients with questionable margins and high grade tumors. Margin status has been shown to be a major predictor of recurrence as well as atypia and location in minor glands (Fonseca).
In one study, the recurrence rate was 36.3% (median disease-free survival 11.34 y), but death was rare with 5-year and 10-year disease-specific survivals of 93.5% and 81.8%, respectively. The most important univariate predictors of recurrence were margin status (P=0.006), angiolymphatic invasion (P=0.002), tumor necrosis (P=0.004), and myoepithelial anaplasia (P=0.038)(Seethala).
Other authors cite lower 5-year and 10-year survival rates of 80% and 72% respectively (Fonseca).
Fonseca I, Soares J (1993). Epithelial-myoepithelial carcinoma of the salivary glands. A study of 22 cases. Virchows Arch A Pathol Anat Histopathol 422: 389-396.
Fonseca I, Felix A, Soares J (2000). Dedifferentiation in salivary gland carcinomas. Am J Surg Pathol 24: 469-471.
Seethala RR, Barnes EL, Hunt JL. Epithelial-myoepithelial carcinoma: a review of the clinicopathologic spectrum and immunophenotypic characteristics in 61 tumors of the salivary glands and upper aerodigestive tract. Am J Surg Pathol. 2007 Jan;31(1):44-57.
Thompson LDR. Endocrine Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier; 2006: 350-4.
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}