
This squamous cell carcinoma presents as a large exophytic fungating mass which circumferentially replaces the cervix. It appears highly friable.
){kind=link}
In the bivalved specimen, the cervix (facing you) is replaced by a fungating exophytic mass which is solid and firm, consistent with extensive desmoplasia found in the tumor.
){kind=link}
Another example of squamous cell carcinoma of the cervix shows an erythematous mass with a finely granular surface afflicting part of the cervical mucosa. The cut surface shows punctate yellow areas of tumor necrosis and a firm, solid tumor.
){kind=link}
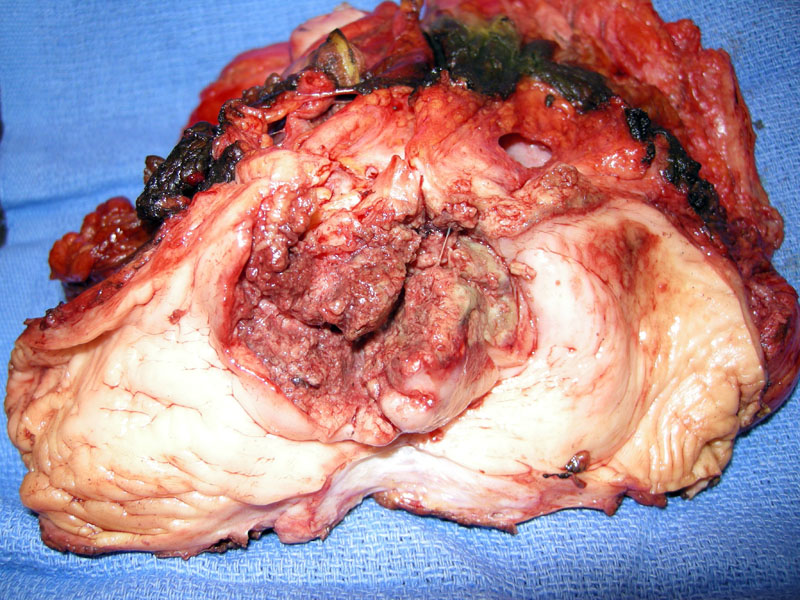
Pelvic exenteration following chemo/radiation shows a cervical neoplasm extending along the endometrial canal and obliterating the normal os.
){kind=link}
The surface epithelium demonstrates high grade dysplasia and overlies nests of invasive squamous cells.
){kind=link}
The invasive squamous cells, which have surrounded an ectatic vessel, are admixed with confluent areas of necrosis, so-called geographic necrosis.
){kind=link}
A different case demonstrates normal glands with underlying diffusely infiltrative tumor cells. Note the gigantic nuclei of some tumor cells, visible even at this low power.
){kind=link}
The wildly pleomorphic cells are indisputably malignant on higher power.
){kind=link}
Invasive nests of squamous cells are seen, surrounded by desmoplastic stroma. Areas of necrosis are present.
){kind=link}
p16 is a surrogate marker for HPV infection, and is strongly positive in HGSIL and cervical cancers. This invasive squamous cell carcinoma demonstrates strong p16 staining.
){kind=link}
The lesional cells demonstrate positivity for keratin 5/6.
){kind=link}
p63 immunostain (positive in SCC) is helpful in distinguishing between squamous cell carcinomas and adenocarcinomas and/or small cell neuroendocrine carcinomas, which show only weak or focal reactivity (Houghton, Wang).
){kind=link}
Squamous cell carcinoma of the cervix is the most common malignancy of the female genital tract worldwide, however, due to successful screening efforts, it is only the third most common malignancy of the female genital tract in the United States. There are approximately 233,000 deaths per year from this disease worldwide, versus 4800 deaths in the United States. It is now firmly established that HPV is the main causal agent, especially HPV type 16. Pre-malignant lesions include LGSIL (low-grade squamous intraepithelial lesions) and HGSIL (high-grade squamous intraepithelial lesions).
Invasive squamous cell carcinomas are divided into three main subtypes (Nucci, Fletcher):
- Keratinizing (well-differentiated): Formation of keratin pearls is key to this subtype. These tumors are usually well-differentiated with pushing borders.
- Large cell non-keratinizing (moderately-differentiated): The tumor cells are still recognizable as squamous cells (large, polygonal with esoinophilic cytoplasm and intercellular bridges), however, keratin pearls are lacking. There is a greater degree of pleomorphism than the keratinizing subtype and the borders tend to be infiltrative, thus, this subtype is generally classified as moderately-differentiated.
- Small cell non-keratinizing (poor-differentiated): The composite tumor cells have a high N/C ratio. Keratinizing features are minimal, and the lesion is poorly-differentiated. To avoid confusion with small cell neuroendocrine carcinoma of the cervix, avoid the words "small cell" is recommended by some experts. Instead, the term "non-keratinizing poorly-differentiated squamous cell carcinoma" is preferred.
Other less common variants of invasive squamous cell carcinoma include: basaloid (not to be confused with adenoid basal carcinoma), verrucous, warty (condylomatous), papillary and lymphoepithelial-like.
Patients with early invasive cancer (stage IA) generally present with an abnormal Pap smear. Postcoital or abnormal vaginal bleeding is the common presentation for stage IB and higher cancers. In advanced disease, pain, hematuria, rectal bleeding and obstructive uropathy results from growth into parametria and involvement of the ureters (Nucci).
Cervical cancers can be treated either surgically or with radiation therapy. Surgical treatments can range from a simple hysterectomy for microinvasive disease to a radical hysterectomy for disease confined to the cervix to an exenteration for advanced pelvic disease. Radiation therapy is usually a combination of teletherapy and brachytherapy with chemosensitization being done with a platinum based agent.
Stage is the single most important prognostic factor. FIGO staging is the most commonly used schema. Briefly, stage I tumors are confined to the uterus, stage II tumors invades beyond the uterus, but not to the pelvic wall or lower third of the vagina, stage III tumors involve the the pelvic wall, lower third of vagina and/or causes kidney dysfunction. Stage IV tumors invades bladder, rectum and/or extends beyond the pelvis.
5-year survivals are as follows: stage IA tumors range from 97-100%, stage IB tumors drops to 84%, stage II tumors range from 65-73%, stage III tumors have less than 15% 5-year survival rates (Fletcher)
→p53 (a homologue p63 tumor suppressor gene) is preferentially expressed in basal and immature cervical squamous epithelium. Thus, it is a good marker to distinguish between cervical SCC and cervical adenocarcinoma (negative P53) and cervical small cell neuroendocrine carcinoma (negative p53).
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 702-4.
Houghton O, McCluggage WG. The expression and diagnostic utility of p63 in the female genital tract. Adv Anat Pathol. 2009 Sep;16(5):316-21.
Nucci MR, Oliva Esther. Gynecologic Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier: 2009: 156-165.
Wang TY, et al. Histologic and immunophenotypic classification of cervical carcinomas by expression of the p53 homologue p63: A study of 250 cases. Human Pathology. Volume 32, Issue 5, Pages 479-486 (May 2001).