
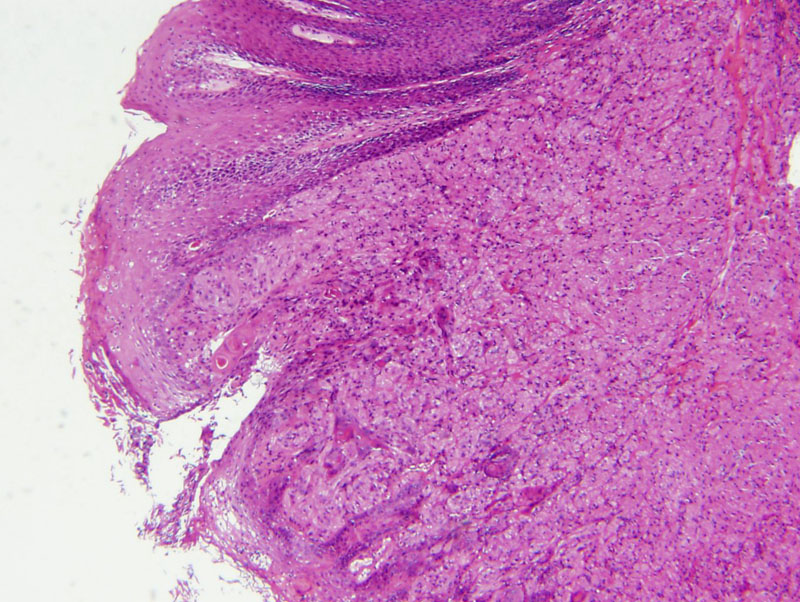
If a GCT grows near an epithelial surface, it may elicit pseudoepitheliomatous hyperplasia. An unsuspecting pathology may be lured into misdiagnosing a superficial biopsy as squamous cell carcinoma. Pseudoepitheliomatous hyperplasia is a very frequent finding in GCT of the larynx and tongue.
){kind=link}
The overlying epithelium may be inflamed with reactive atypia.
){kind=link}
The tumor cells are large polygonal cells with abundant pale granular cytoplasm. Mitotic activity and pleomorphism areusually absent.
){kind=link}
The nuclei are small and either eccentrically or centrally located. A delicate fibrovascular stroma is seen separating the tumor cells. Note the coarse granular cytoplasm for which the tumor was named.
){kind=link}
Granular cell tumors (GCT) are benign neoplasms that can occur in virtually every tissue and organ. The most common anatomic sites are tongue, skin/subcutaneous tissue, oral cavity and larynx. Other sites include the GI tract, where the esophagus and large intestine are the common frequently affected.
The neoplastic cells are believed to be Schwannian in origin, which is supported by IHC studies that demonstrate positivity for S-100 and NSE (neuron-specific enolase). Additionally, the granules within the tumor cells are PAS-positive and diastase-resistant.
Grossly, these tumors are nodular (less than 4 cm in diameter) with ill-defined margins and a tan-yellow homogenous cut surface. Microscopically, the granular cells have abundant coarsely granular cytoplasm with small nuclei. The cells are bland and monomorphic. If pleomorphism, mitoses and necrosis is seen, one must consider the very rare diagnosis of a GCT with malignant potential.
30-50% of GCT occur in the head and neck region, with the most common site being the tongue. Presentation depends on the location and size of the tumor. Larger tumors in the larynx may cause stridor and dysphagia.
GCT occurs over a wide age range; peak incidence is between 40-50 years of age. There is a female preponderance (2:1) and interestingly, 2/3 of patients are black.
Excellent; only 2-8% recur even after incomplete excision. Note that there is a very rare subset of GCT with malignant potential. Although no established criteria current exist, increased mitotic activity, necrosis and pleomorphism may suggest a more aggressive tumor.
1 Thomspon LDR. Endocrine Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier; 2006: 38-43.
2 Mills SE, Gaffey MJ, Frierson HF. Tumors of the Upper Aerodigestive Tract and Ear: Atlas of Tumor Pathology. Third Series, Fascicle 26. Washington DC; AFIP: 1997: 139-144.