System: Gastrointestinal: Colon: Benign: Juvenile Polyp

System: Gastrointestinal: Colon: Benign: Juvenile Polyp

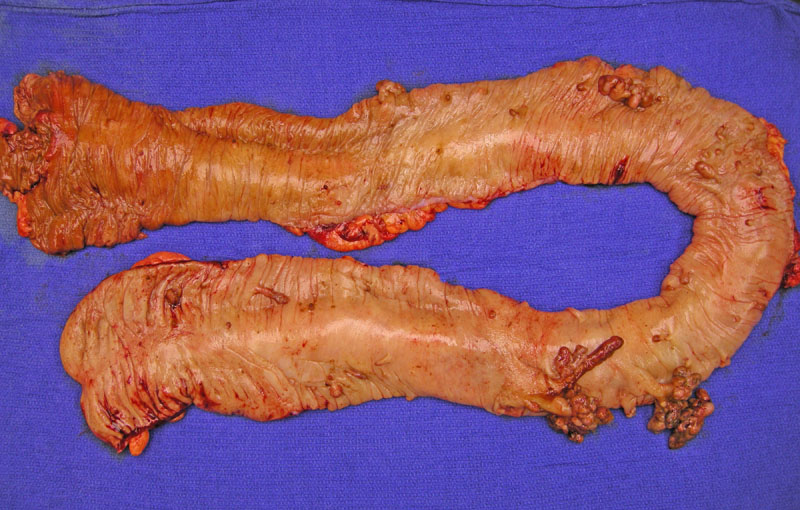
This colectomy from a patient with juvenile polyposis shows scattered pedunculated and sessile polyps. Grossly, juvenile polyps tend to be large (1-3 cm), rounded polyps and pedunculated but may occasionally be sessile. The surface is frequently eroded.
Histologically, the lamina propria is expanded and encloses cystically dilated glands. Juvenile polyps are frequently misdiagnosed as inflammatory polyps (mucosal prolapse syndrome). A lack of smooth muscle proliferation in the lamina propria and a strikingly prominent lamina propria in juvenile polyps are helpful features to distinguish between these two entities.
A proliferation of variably sized mucus glands with cystic structures is encased in abundant lamina propria. The lamina propria contains acute and chronic inflammatory cells and congested vessels. Note the surface erosion and granulation tissue.
Cystically dilated glands containing cellular debris are a characteristic finding.
In this different polyp, a proliferation of bland (non-malignant) glands fill the deeper portions of the polyp
The surface shows lamina propria edema and chronic inflammatory cells with glandular distortion.
Yet another image of surface erosion, which is common.
Variable sized glands are lined by mucus-secreting cells. The lining cells may be attentuated (bottom of image) due to pressure from cystic fluid.
The hamartomatous polyposis syndromes are an interesting group of disorders which have in common relatively benign hamartomatous polyps of the GI tract, but also carry an increased risk of cancer. Hamartomatous polyps are discrete proliferations of cellular components native to the tissue of origin. In the GI tract, they appear as malformations of glands and lamina propria. Polyps of the various hamartomatous polyposis syndromes exhibit characteristic histology.
The three most common hamartomatous polyposis syndromes are: Peutz-Jeghers Syndrome (PJS), Juvenile Polyposis Syndrome (JPS) and PTEN hamartoma tumor syndrome (Gammon). The progression of these polyps to cancer is poorly understood, and represents a different pathway than that of adenomatous polyposis. The genetic mutations responsible for these syndromes have largely been elucidated, and it is important to identify patients affected by these conditions as to appropriately monitor intestinal and extra-intestinal complications.
Sporadic juvenile polyps are not uncommon and may be found in up to 2% of children. When these isolated polyps are identified in adults, they are termed "retention polyps". These sporadic lesions are generally asymptomatic and are not related to JPS.
The criteria for JPS are: (1) greater than 5 juvenile polyps in the colon (2) presence of extracolonic juvenile polyps (3) any number of juvenile polyps in a patient with a family history of JPS (Iacobuzio-Donahue). Usually in JPS, numerous (50-100) hamartomatous polyps are found in the GI tract (Kumar).
Up to 50% of JPS arise de novo, and the rest are inherited in an autosomal dominant manner. Thus far, two genes have been associated with JPS: SMAD4 and BMPRIA, which are involved in cell cycle regulation. Testing for deletions or point mutations in these genes may now be offered to patients (Gammon)
Average age at diagnosis is 9.5 years for JPS, although sporadic lesions may be found at an earlier age. Most common presentation is painless rectal bleeding. 10-20% of patients experience abdominal pain, protrusion of the polyp through the anus and diarrhea. In rare cases of extensive polyposis, there may be intussusception, protein-losing enteropathy and malabsorption (Iacobuzio-Donahue).
Dyplasia has been identified in up to 30% of polyps in JPS patients, thus, these patients require vigilant colorectal surveillance starting at young age. The incidence of colon cancer is 20% by age 35 and 68% by age 68. For patients with gastric polyps, the incidence of gastric carcinoma is 21% (Schreibman).
Colonoscopy and upper endoscopy is recommended starting at age 15, to be repeated annually or every two years (depending on previous colonoscopy and endoscopy findings and clinical symptoms)(Gammon). Patients with extensive polyposis may require a colectomy.
A 2007 study conducted by Brosens and colleagues on 84 patients with JPS found the relative risk colorectal cancer was 34.0 compared to the general population. The lifetime risk was 38.7% and the average age at diagnosis was 43.9 (Brosens).
→Sporadic juvenile polyps are not uncommon and does not indicate a diagnosis of JPS.
→Microscopically, tortuous and dilated glands are embedded in an inflammed stroma.
→The most common clinical presentation is painless bleeding.
→It is important to recognize JPS as these patients have an increased risk of developing colon cancer at an earlier age.
• Stomach : Peutz-Jeugers Polyp
Brosens LA, et al. Risk of colorectal cancer in juvenile polyposis. Gut. 2007;56(7):965-7.
Gammon A, Jasperson K, Kolhmann W, et al. Hamartomatous polyposis syndrome. Best Practice and Research Clinical Gastroenterology. 23 (2009); 219-231.
Iacobuzio-Donahue CA, Montgomery EA. Gastrointestinal and Liver Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier; 2005: 355-358.
Kumar V, Abbas AK, Fausto N. Robbins and Cotran Pathologic Basis of Disease. 7th Ed. Philadelphia, PA: Elsevier; 2005: 859.
Mills SE, ed. Sternberg's Diagnostic Surgical Pathology.4th Ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2004: 1550.
Schreibman IR, Baker M, Amos C. The Hamartomatosis Polyposis Syndromes: A Clinical and Molecular Review. Am J Gastroenterol. 2005;100:476-490.
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}